

Exploring the burden of inpatient readmissions after major cancer surgery
- PMID: 25547502
- PMCID: PMC4314594
- DOI: 10.1200/JCO.2014.55.5938
Exploring the burden of inpatient readmissions after major cancer surgery
Abstract
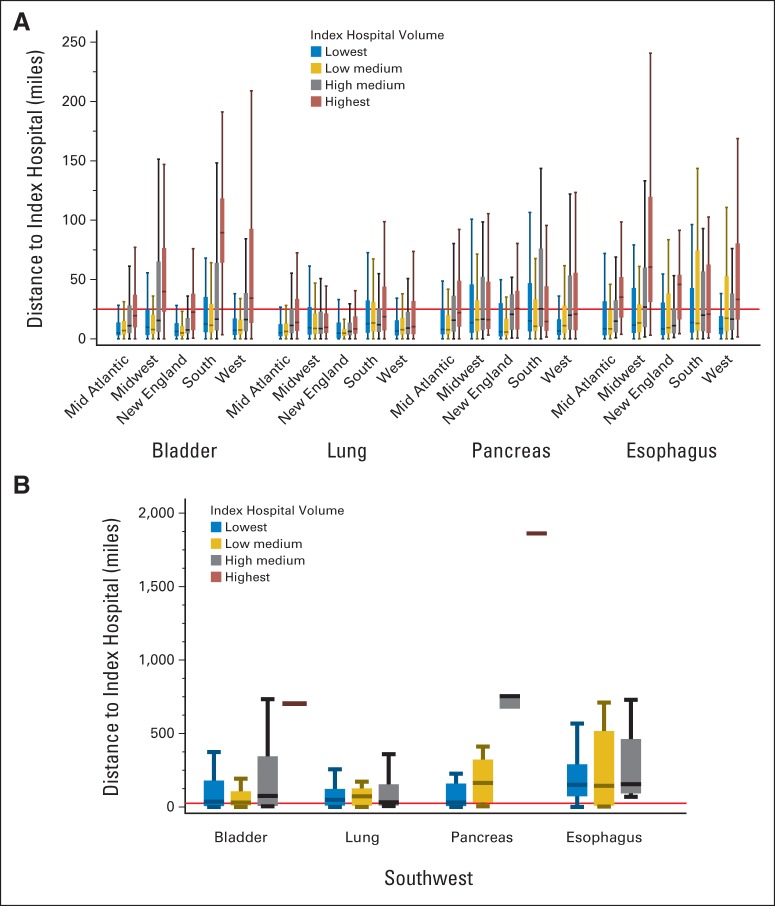
Purpose: Travel distances to care have increased substantially with centralization of complex cancer procedures at high-volume centers. We hypothesize that longer travel distances are associated with higher rates of postoperative readmission and poorer outcomes.
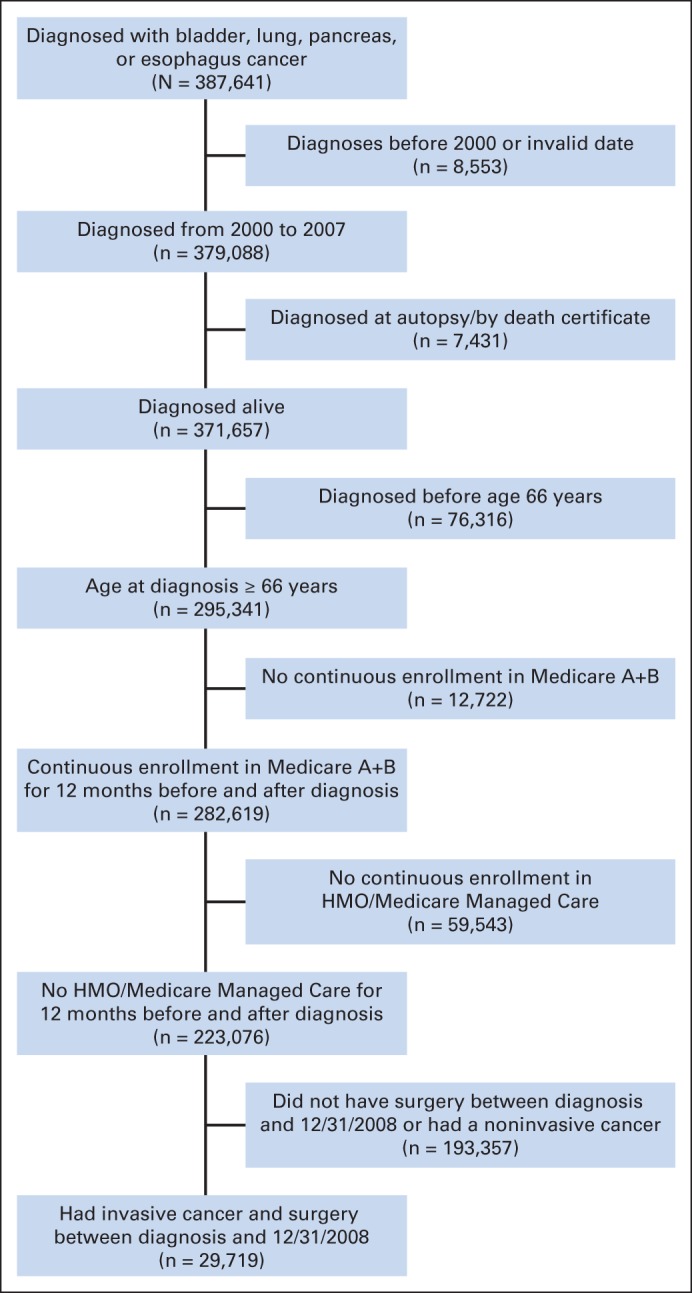
Methods: SEER-Medicare patients with bladder, lung, pancreas, or esophagus cancer who were diagnosed in 2001 to 2007 and underwent extirpative surgery were included. Readmission rates and survival were calculated using Kaplan-Meier functions. Multivariable negative binomial models were used to examine factors associated with readmission.
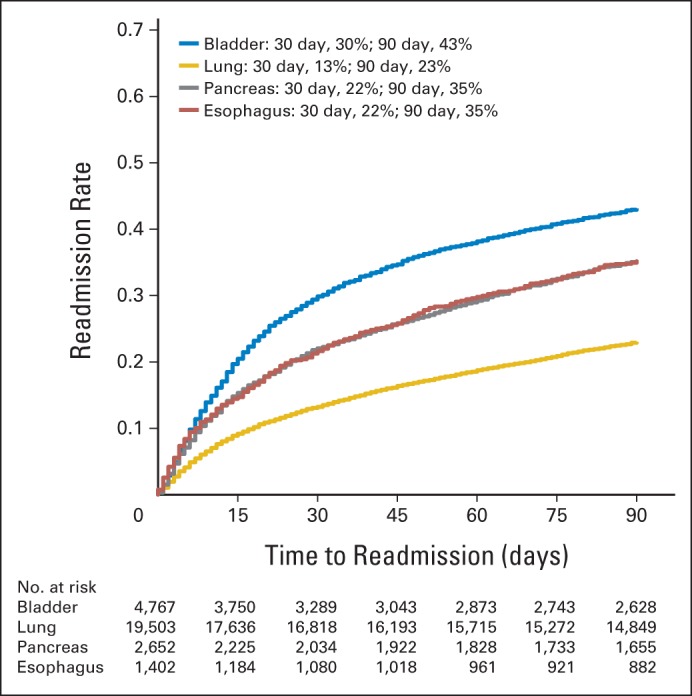
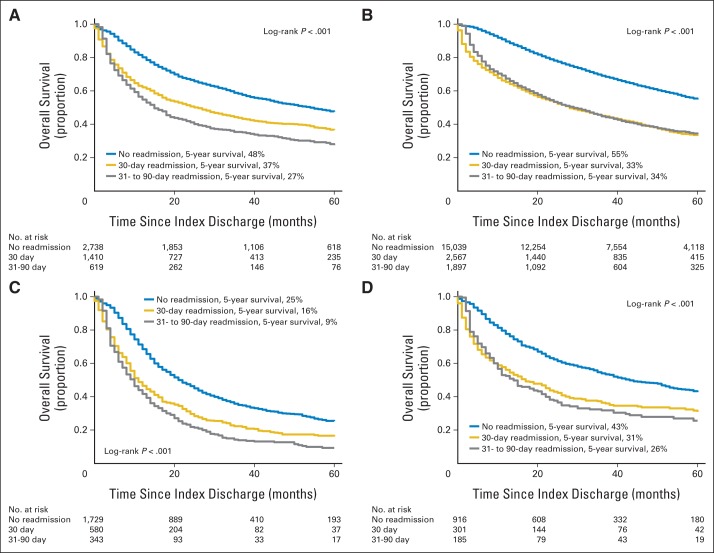
Results: Four thousand nine hundred forty cystectomies, 1,573 esophagectomies, 20,362 lung resections, and 2,844 pancreatectomies were included. Thirty- and 90-day readmission rates ranged from 13% to 29% and 23% to 43%, respectively, based on tumor type. Predictors of readmission were discharge to somewhere other than home, longer length of stay, comorbidities, higher stage at diagnosis, and longer travel distance (P < .001 for each). Patients who lived farther from the index hospital also had increased emergency room visits and were more likely to be readmitted to a hospital other than the index hospital (P < .001). Of readmitted patients, 31.9% were readmitted more than once. Long-term survival was worse and costs of care higher for patients who were readmitted (P < .001 for all).
Conclusion: The burden of readmissions after major cancer surgery is high, resulting in substantially poorer patient outcomes and higher costs. Risk of readmission was most strongly associated with length of stay and discharge destination. Travel distance also has an impact on patterns of readmission. Interventions targeted at higher risk individuals could potentially decrease the population burden of readmissions after major cancer surgery.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
Reply to G.J. Weiss.J Clin Oncol. 2015 Jul 1;33(19):2229-30. doi: 10.1200/JCO.2015.62.1359. Epub 2015 May 26. J Clin Oncol. 2015. PMID: 26014297 No abstract available.
-
Influence of Robotic-Assisted Surgery on Readmission Burden.J Clin Oncol. 2015 Jul 1;33(19):2229. doi: 10.1200/JCO.2015.61.7464. Epub 2015 May 26. J Clin Oncol. 2015. PMID: 26014299 No abstract available.
-
Re: Exploring the Burden of Inpatient Readmissions after Major Cancer Surgery.J Urol. 2015 Oct;194(4):1068. doi: 10.1016/j.juro.2015.06.008. Epub 2015 Jun 9. J Urol. 2015. PMID: 26382809 No abstract available.
References
-
- Donat SM, Shabsigh A, Savage C, et al. Potential impact of postoperative early complications on the timing of adjuvant chemotherapy in patients undergoing radical cystectomy: A high-volume tertiary cancer center experience. Eur Urol. 2009;55:177–185. - PubMed
-
- Yermilov I, Bentrem D, Sekeris E, et al. Readmissions following pancreaticoduodenectomy for pancreas cancer: A population-based appraisal. Ann Surg Oncol. 2009;16:554–561. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
