

Applicability of preoperative nuclear morphometry to evaluating risk for cervical lymph node metastasis in oral squamous cell carcinoma
- PMID: 25549090
- PMCID: PMC4280216
- DOI: 10.1371/journal.pone.0116452
Applicability of preoperative nuclear morphometry to evaluating risk for cervical lymph node metastasis in oral squamous cell carcinoma
Abstract
Background: We previously reported the utility of preoperative nuclear morphometry for evaluating risk for cervical lymph node metastases in tongue squamous cell carcinoma. The risk for lymph node metastasis in oral squamous cell carcinoma, however, is known to differ depending on the anatomical site of the primary tumor, such as the tongue, gingiva, mouth floor, and buccal mucosa. In this study, we evaluated the applicability of this morphometric technique to evaluating the risk for cervical lymph node metastasis in oral squamous cell carcinoma.
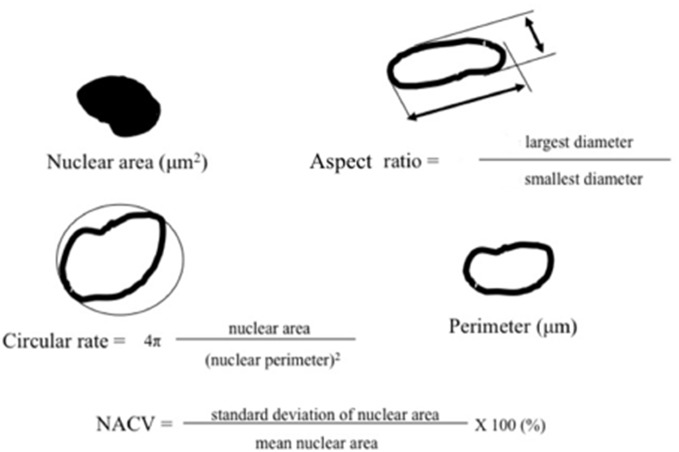
Methods: A digital image system was used to measure the mean nuclear area, mean nuclear perimeter, nuclear circular rate, ratio of nuclear length to width (aspect ratio), and nuclear area coefficient of variation (NACV). Relationships between these parameters and nodal status were evaluated by t-test and logistic regression analysis.
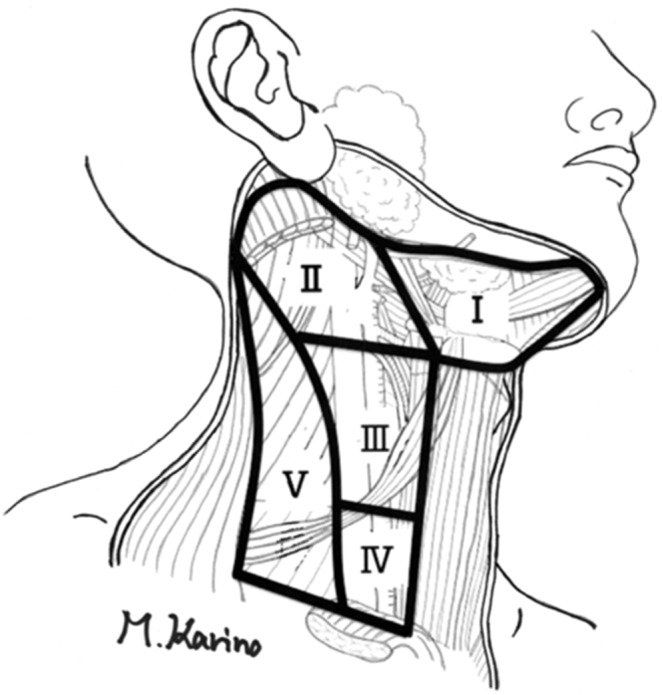
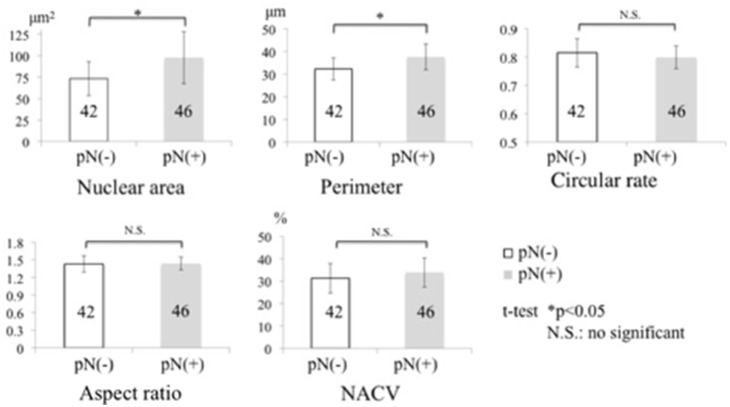
Results: Eighty-eight cases of squamous cell carcinoma (52 of the tongue, 25 of the gingiva, 4 of the buccal mucosa, and 7 of the mouth floor) were included: 46 with positive node classification and 42 with negative node classification. Nuclear area and perimeter were significantly larger in node-positive cases than in node-negative cases; however, there were no significant differences in circular rate, aspect ratio, or NACV. We derived two risk models based on the results of multivariate analysis: Model 1, which identified age and mean nuclear area and Model 2, which identified age and mean nuclear perimeter. It should be noted that primary tumor site was not associated the pN-positive status. There were no significant differences in pathological nodal status by aspect ratio, NACV, or primary tumor site.
Conclusion: Our method of preoperative nuclear morphometry may contribute valuable information to evaluations of the risk for lymph node metastasis in oral squamous cell carcinoma.
Conflict of interest statement
Figures
References
-
- Kim KY, Cha IH (2011) A novel algorithm for lymph node status prediction of oral cancer before surgery. Oral Oncol 47:1069–1073. - PubMed
-
- Lim YC, Koo BS, Lee JS, Choi EC (2006) Level V lymph node dissection in oral and oropharyngeal carcinoma patients with clinically node-positive neck: Is it absolutely necessary? Laryngoscope 116:1232–1235. - PubMed
-
- Montes DM, Carlson ER, Fernandes R, Ghali GE, Lubek J, et al. (2011) Oral maxillary squamous carcinoma: an indication for neck dissection in the clinically negative neck. Head Neck 33:1581–1585. - PubMed
-
- Liao CT, Hsueh C, Lee LY, Lin CY, Fan KH, et al. (2012) Neck dissection field and lymph node density predict prognosis in patients with oral cavity cancer and pathological node metastases treated with adjuvant therapy. Oral Oncol 48:329–336. - PubMed
-
- Hoch S, Fasunla J, Eivazi B, Werner JA, Teymoortash A. (2012) Delayed lymph node metastases after elective neck dissection in patients with oral and oropharyngeal cancer and pN0 neck. Am J Otolaryngol 33:505–509. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
