

Traumatic carotid-rosenthal fistula treated with Jostent Graftmaster
- PMID: 25550998
- PMCID: PMC4278154
- DOI: 10.4329/wjr.v6.i12.924
Traumatic carotid-rosenthal fistula treated with Jostent Graftmaster
Abstract
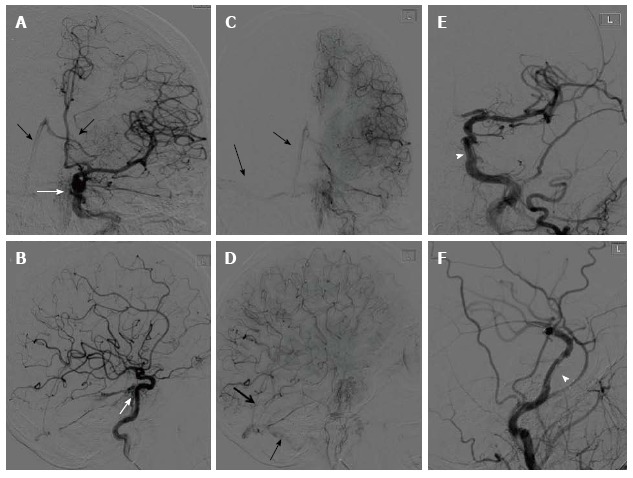
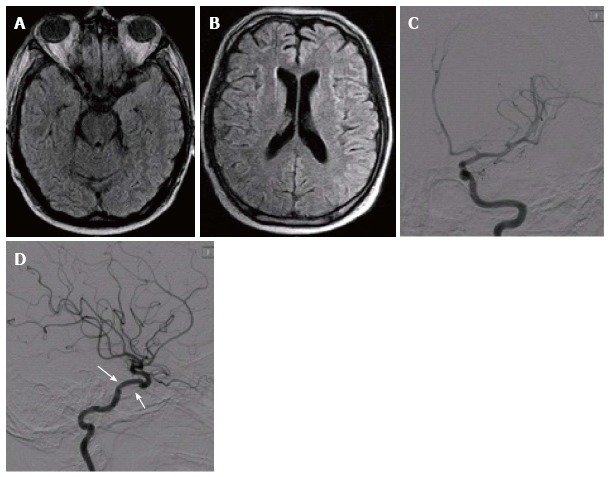
Traumatic injuries of the carotid artery may result in severe morbidity and mortality. The most common location of carotid artery injury is the cavernous segment, which may result in fistulous connection to the cavernous sinus and ophthalmic veins, which in turn lead to pressure symptoms in the ipsilateral orbit. Unlike the commonly reported direct traumatic carotid-cavernous fistula, we describe an unusual case of a 38-year-old man presented with a traumatic brain injury led to a fistula connection between the cavernous carotid artery and the ipsilateral basal vein of Rosenthal, with eventual drainage to the straight and transverse sinuses. The basal vein of Rosenthal is usually formed from confluence of anterior and middle cerebral veins deep in the Sylvian fissure and drain the insular cortex and the cerebral peduncles to the vein of Galen. Immediate endovascular deployment of a covered stent in the cavernous carotid artery allowed sealing the laceration site. Three months follow up showed a non-focal neurological examination and healed carotid laceration over the covered stent.
Keywords: Carotid artery; Fracture; Jostent; Skull base; Trauma.
Figures
References
-
- Sliker CW. Blunt cerebrovascular injuries: imaging with multidetector CT angiography. Radiographics. 2008;28:1689–1708; discussion 1709-1710. - PubMed
-
- Sun GH, Shoman NM, Samy RN, Pensak ML. Analysis of carotid artery injury in patients with basilar skull fractures. Otol Neurotol. 2011;32:882–886. - PubMed
-
- Ellis JA, Goldstein H, Connolly ES, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32:E9. - PubMed
-
- Crawford SC, Digre KB, Palmer CA, Bell DA, Osborn AG. Thrombosis of the deep venous drainage of the brain in adults. Analysis of seven cases with review of the literature. Arch Neurol. 1995;52:1101–1108. - PubMed
-
- Gemmete JJ, Chaudhary N, Pandey A, Ansari S. Treatment of carotid cavernous fistulas. Curr Treat Options Neurol. 2010;12:43–53. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
