

A meta-analysis to derive literature-based benchmarks for readmission and hospital mortality after patient discharge from intensive care
- PMID: 25551448
- PMCID: PMC4312433
- DOI: 10.1186/s13054-014-0715-6
A meta-analysis to derive literature-based benchmarks for readmission and hospital mortality after patient discharge from intensive care
Abstract
Introduction: We sought to derive literature-based summary estimates of readmission to the ICU and hospital mortality among patients discharged alive from the ICU.
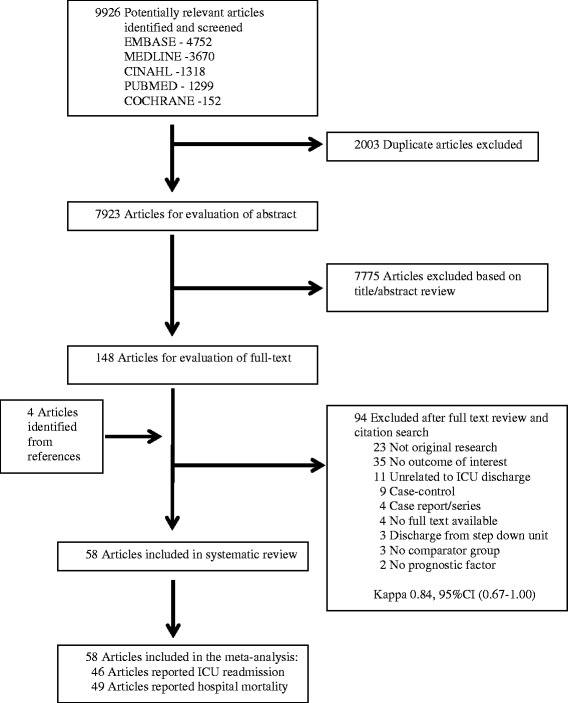
Methods: We searched MEDLINE, Embase, CINAHL and the Cochrane Central Register of Controlled Trials from inception to March 2013, as well as the reference lists in the publications of the included studies. We selected cohort studies of ICU discharge prognostic factors that in which readmission to the ICU or hospital mortality among patients discharged alive from the ICU was reported. Two reviewers independently abstracted the number of patients readmitted to the ICU and hospital deaths among patients discharged alive from the ICU. Fixed effects and random effects models were used to estimate the pooled cumulative incidence of ICU readmission and the pooled cumulative incidence of hospital mortality.
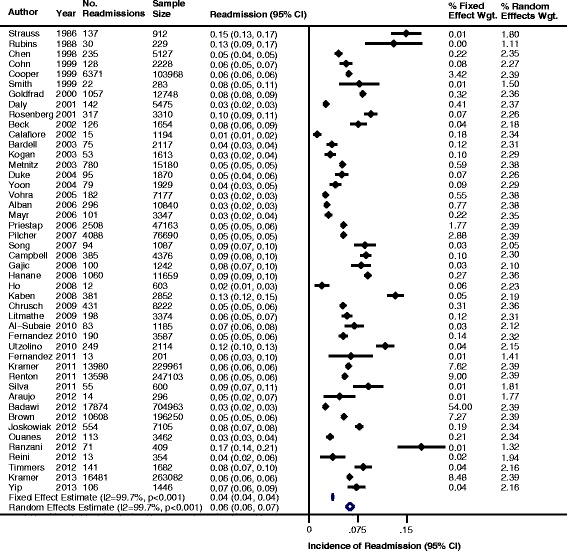
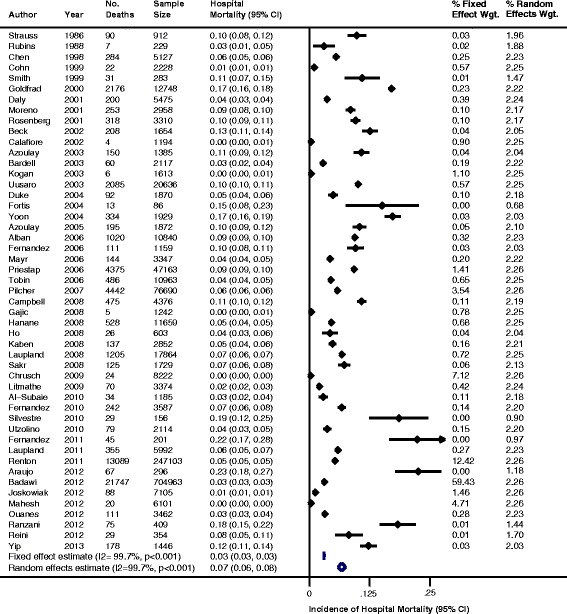
Results: The analysis included 58 studies (n = 2,073,170 patients). The majority of studies followed patients until hospital discharge (n = 46 studies) and reported readmission to the ICU (n = 46 studies) or hospital mortality (n = 49 studies). The cumulative incidence of ICU readmission was 4.0 readmissions (95% confidence interval (CI), 3.9 to 4.0) per 100 patient discharges using fixed effects pooling and 6.3 readmissions (95% CI, 5.6 to 6.9) per 100 patient discharges using random effects pooling. The cumulative incidence of hospital mortality was 3.3 deaths (95% CI, 3.3 to 3.3) per 100 patient discharges using fixed effects pooling and 6.8 deaths (95% CI, 6.1 to 7.6) per 100 patient discharges using random effects pooling. There was significant heterogeneity for the pooled estimates, which was partially explained by patient, institution and study methodological characteristics.
Conclusions: Using current literature estimates, for every 100 patients discharged alive from the ICU, between 4 and 6 patients on average will be readmitted to the ICU and between 3 and 7 patients on average will die prior to hospital discharge. These estimates can inform the selection of benchmarks for quality metrics of transitions of patient care between the ICU and the hospital ward.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
