

Protective effects of (1-(4-hydroxy-phenyl)-3-m-tolyl-propenone chalcone in indomethacin-induced gastric erosive damage in rats
- PMID: 25551777
- PMCID: PMC4339009
- DOI: 10.1186/s12917-014-0303-7
Protective effects of (1-(4-hydroxy-phenyl)-3-m-tolyl-propenone chalcone in indomethacin-induced gastric erosive damage in rats
Abstract
Background: Non-steroidal anti-inflammatory drugs (NSAIDs) can result in peptic ulcer disease (PUD) which is a common condition worldwide. The aim of this study was to evaluate the antiulcer properties of (1-(4-hydroxy-phenyl)-3-m-tolyl-propenone) (HPTP) chalcone in rats using indomethacin as ulcerogenic agent.
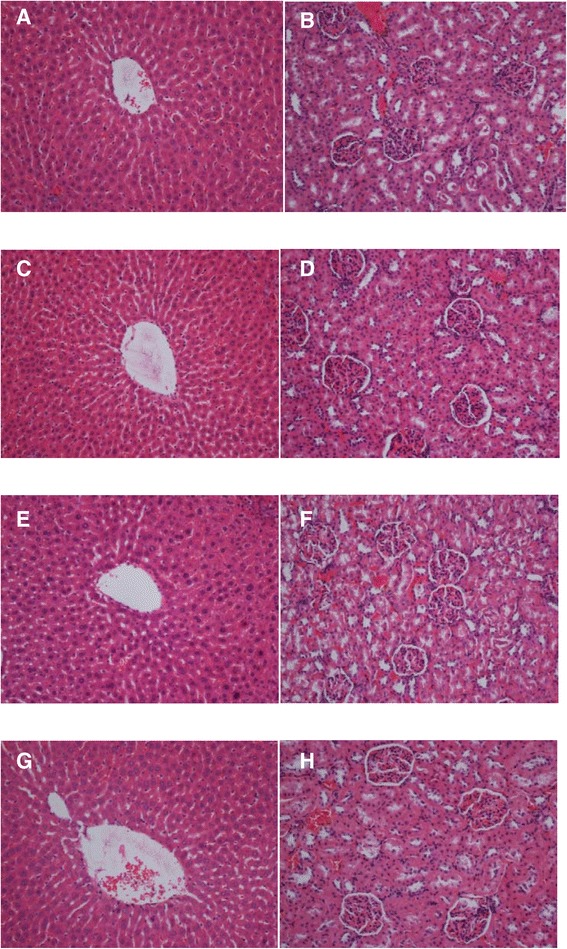
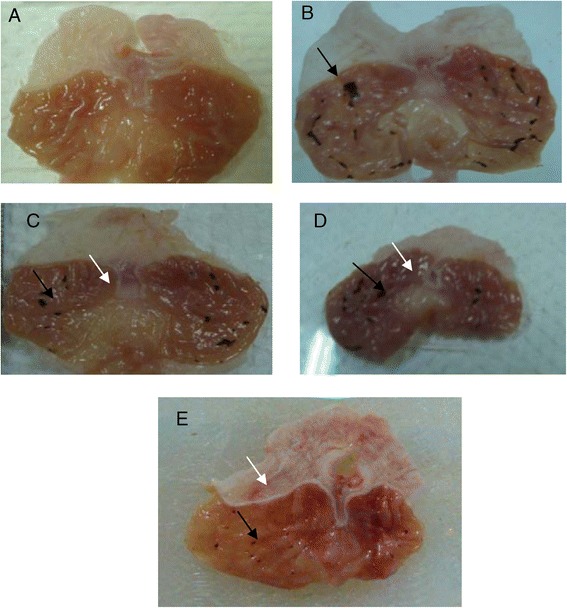
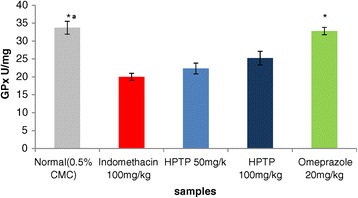
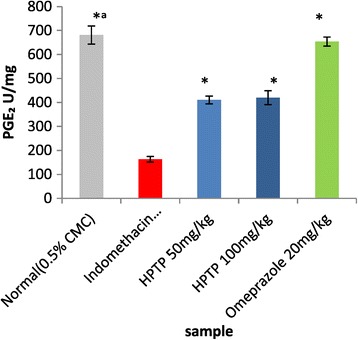
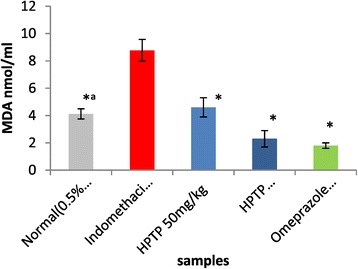
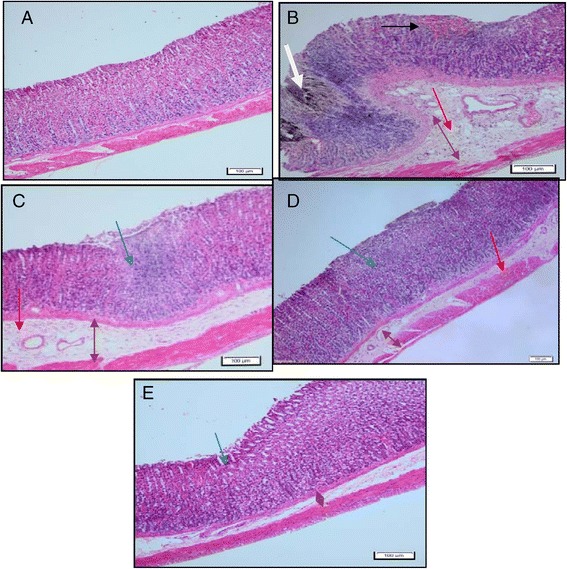
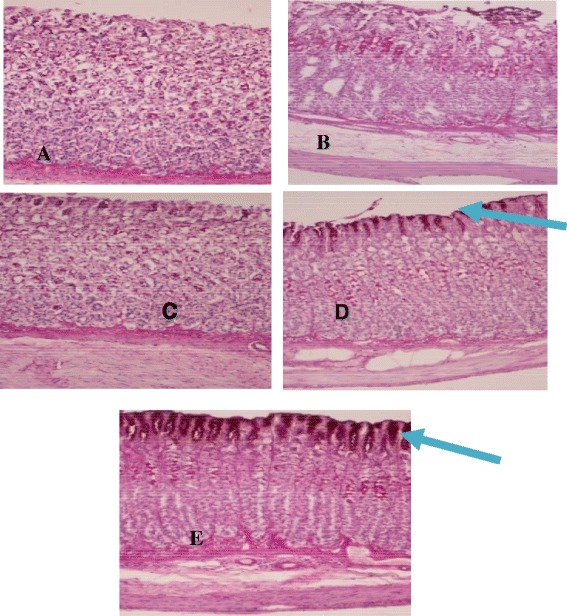
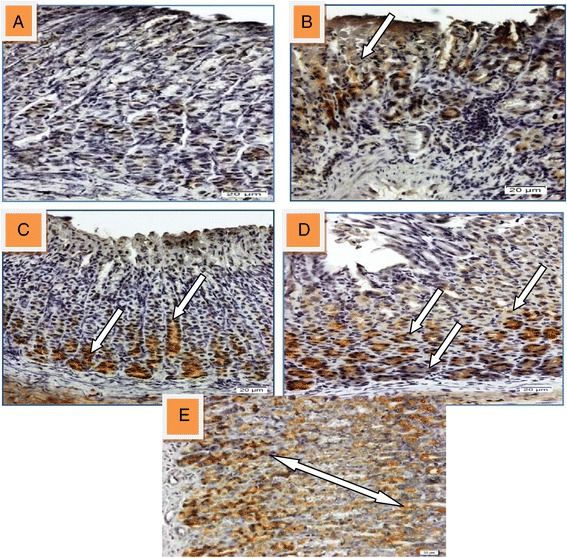
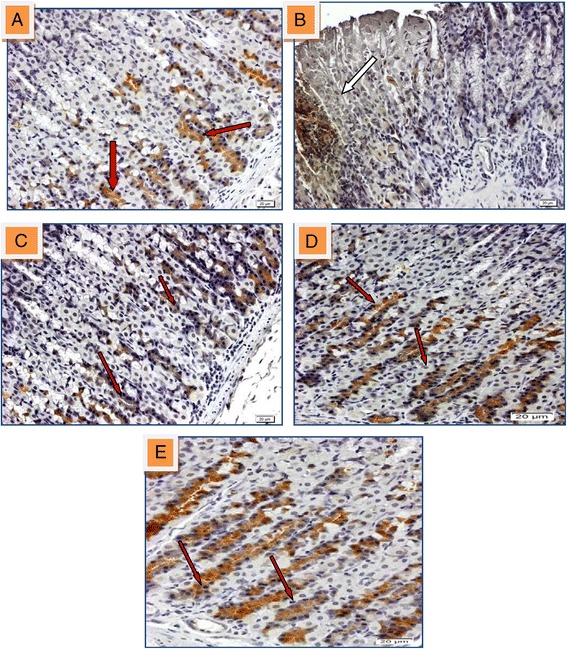
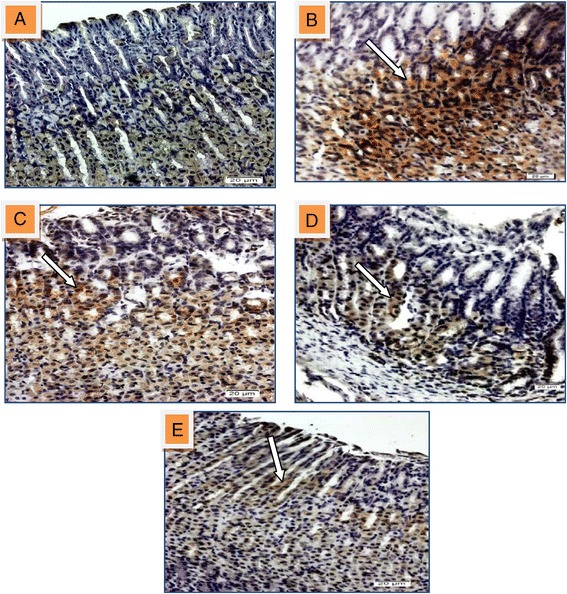
Results: None of the rats showed symptoms of kidney and liver toxicity during the term of the study. Administration of HPTP had decreased the acidity, increased gastric wall mucus and flattening of gastric mucosa and reducing erosive gastric damage area. HPTP also showed dose dependent increase in SOD, GPx activity and PGE2 level and decrease MDA. H & E stain showed decreased infiltration of leucocytes with edema of submucosal layer. PAS staining showed intense uptake of magenta color of gastric wall mucus in rats fed with HPTP, and immunohistochemical staining of gastric mucosa revealed over-expression of HSP70 protein, down-expression of Bax protein and over expression of TGF-β in rats administered with HPTP.
Conclusion: This study has revealed that chalcone1-(4-hydroxy-phenyl)-3-m-tolyl-propenone can serve as a safe and effective antiulcer agent as it has been proved to increase pH and gastric wall mucus, increase GPx, SOD, PGE2, and decrease MDA level, ultimately, it has also contributes towards the over-expression of HSP protein andTGF-β, and down-expression of Bax protein.
Figures

Similar articles
-
Gastric antisecretory and antiulcer activities of Cyclea peltata (Lam.) Hook. f. & Thoms. in rats.J Ethnopharmacol. 2009 Sep 7;125(2):350-5. doi: 10.1016/j.jep.2009.04.039. Epub 2009 May 4. J Ethnopharmacol. 2009. PMID: 19397987
-
Gastric anti-ulcer and cytoprotective effect of l-serine in rats.Res Commun Mol Pathol Pharmacol. 1997 Aug;97(2):171-84. Res Commun Mol Pathol Pharmacol. 1997. PMID: 9344230
-
Different mechanisms in formation and prevention of indomethacin-induced gastric ulcers.Inflammation. 2010 Aug;33(4):224-34. doi: 10.1007/s10753-009-9176-5. Inflammation. 2010. PMID: 20084447 Review.
-
15-PGDH inhibitors: the antiulcer effects of carbenoxolone, pioglitazone and verapamil in indomethacin induced peptic ulcer rats.Eur Rev Med Pharmacol Sci. 2013;17(15):2000-9. Eur Rev Med Pharmacol Sci. 2013. PMID: 23884819
-
[New therapeutic approaches to peptic ulcer using mucosal protective agents].Nihon Rinsho. 2002 Feb;60 Suppl 2:377-81. Nihon Rinsho. 2002. PMID: 11979810 Review. Japanese. No abstract available.
Cited by
-
Synthesis, In Silico and In Vitro Evaluation for Acetylcholinesterase and BACE-1 Inhibitory Activity of Some N-Substituted-4-Phenothiazine-Chalcones.Molecules. 2020 Aug 27;25(17):3916. doi: 10.3390/molecules25173916. Molecules. 2020. PMID: 32867308 Free PMC article.
-
The therapeutic potential of Salvia aegyptiaca extracts in ethanol-induced gastric ulcer: insights into macroscopic, histopathological, and biochemical mechanisms.Turk J Biol. 2024 Dec 2;49(1):40-51. doi: 10.55730/1300-0152.2722. eCollection 2025. Turk J Biol. 2024. PMID: 40104582 Free PMC article.
-
The ameliorative effects of cinnamon oil against ethanol-induced gastric ulcer in rats by regulating oxidative stress and promoting angiogenesis.J Mol Histol. 2022 Jun;53(3):573-587. doi: 10.1007/s10735-022-10072-y. Epub 2022 Mar 15. J Mol Histol. 2022. PMID: 35290563
-
Gastroprotective potential of methanolic extract and dimethyl cardamonin from Campomanesia reitziana fruits in mice.Naunyn Schmiedebergs Arch Pharmacol. 2017 Jun;390(6):661-666. doi: 10.1007/s00210-017-1369-0. Epub 2017 Apr 1. Naunyn Schmiedebergs Arch Pharmacol. 2017. PMID: 28365824
-
Prophylactic effects of Clausena excavata Burum. f. leaf extract in ethanol-induced gastric ulcers.Drug Des Devel Ther. 2016 Jun 15;10:1973-86. doi: 10.2147/DDDT.S103993. eCollection 2016. Drug Des Devel Ther. 2016. PMID: 27366052 Free PMC article.
References
-
- Chan FK, Abraham NS, Scheiman JM, Laine L. Management of patients on nonsteroidal anti-inflammatory drugs: a clinical practice recommendation from the First International Working Party on Gastrointestinal and Cardiovascular Effects of Nonsteroidal Anti-inflammatory Drugs and Anti-platelet Agents. Am J Gastroenterol. 2008;103(11):2908–2918. doi: 10.1111/j.1572-0241.2008.02200.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
