

Coronary microvascular rarefaction and myocardial fibrosis in heart failure with preserved ejection fraction
- PMID: 25552356
- PMCID: PMC4324362
- DOI: 10.1161/CIRCULATIONAHA.114.009625
Coronary microvascular rarefaction and myocardial fibrosis in heart failure with preserved ejection fraction
Abstract
Background: Characterization of myocardial structural changes in heart failure with preserved ejection fraction (HFpEF) has been hindered by the limited availability of human cardiac tissue. Cardiac hypertrophy, coronary artery disease (CAD), coronary microvascular rarefaction, and myocardial fibrosis may contribute to HFpEF pathophysiology.
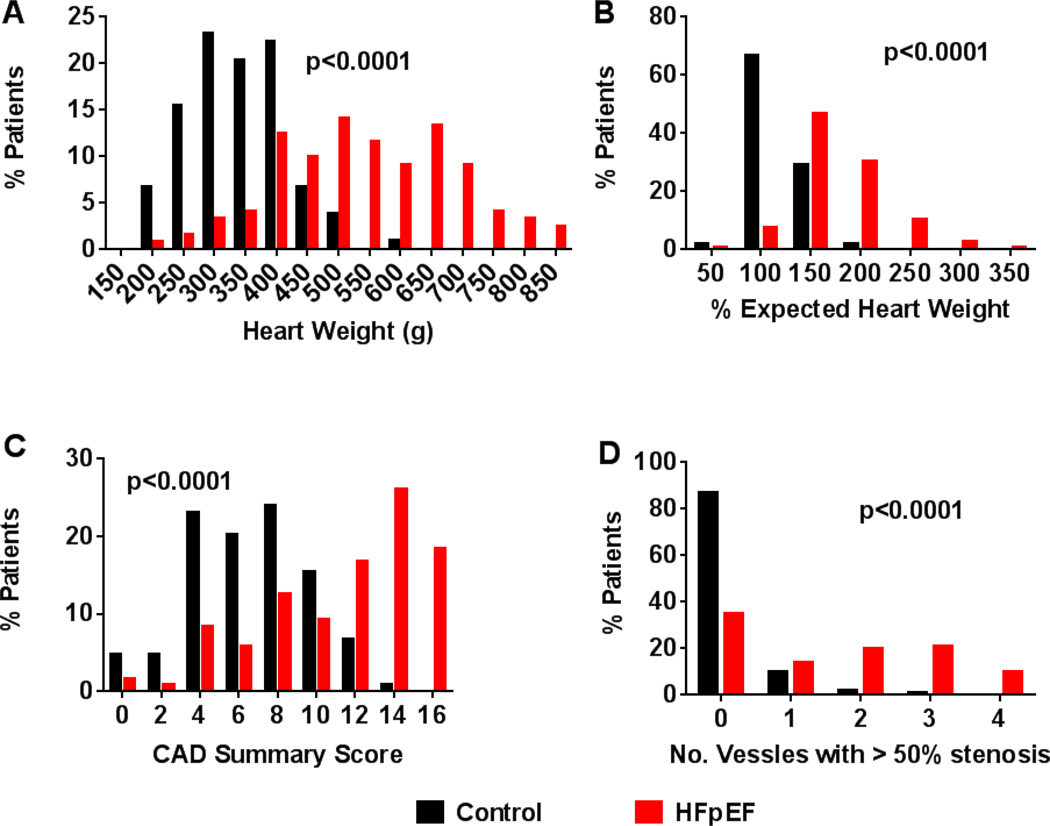
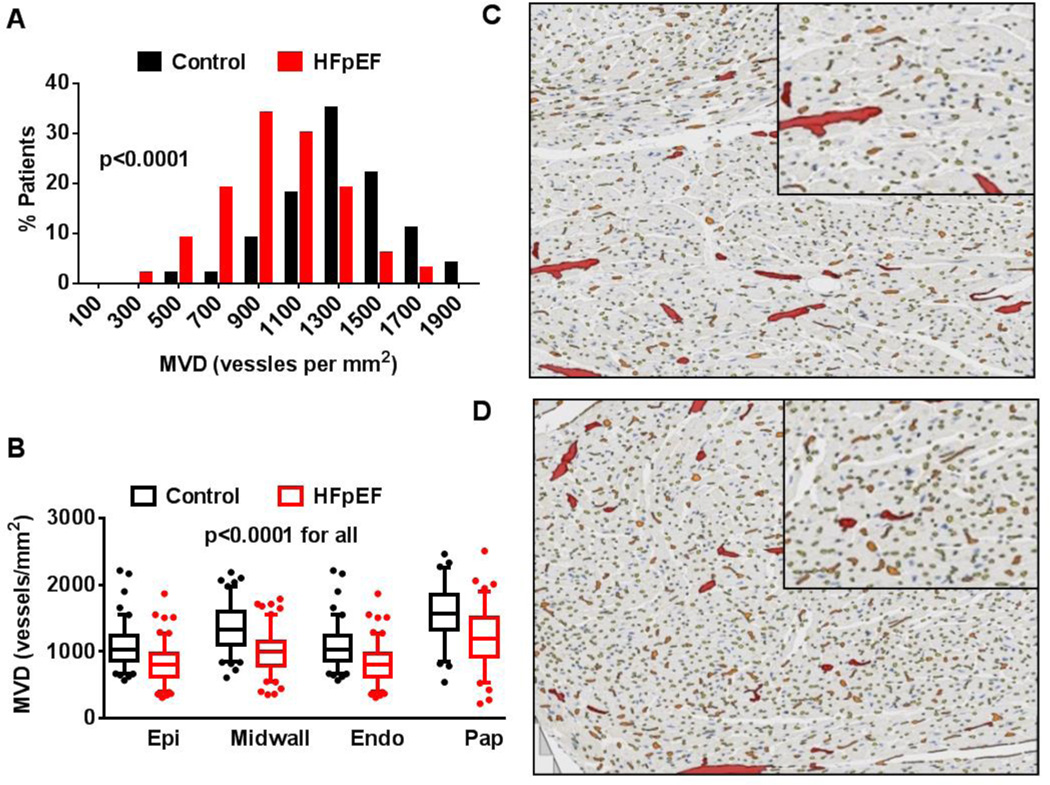
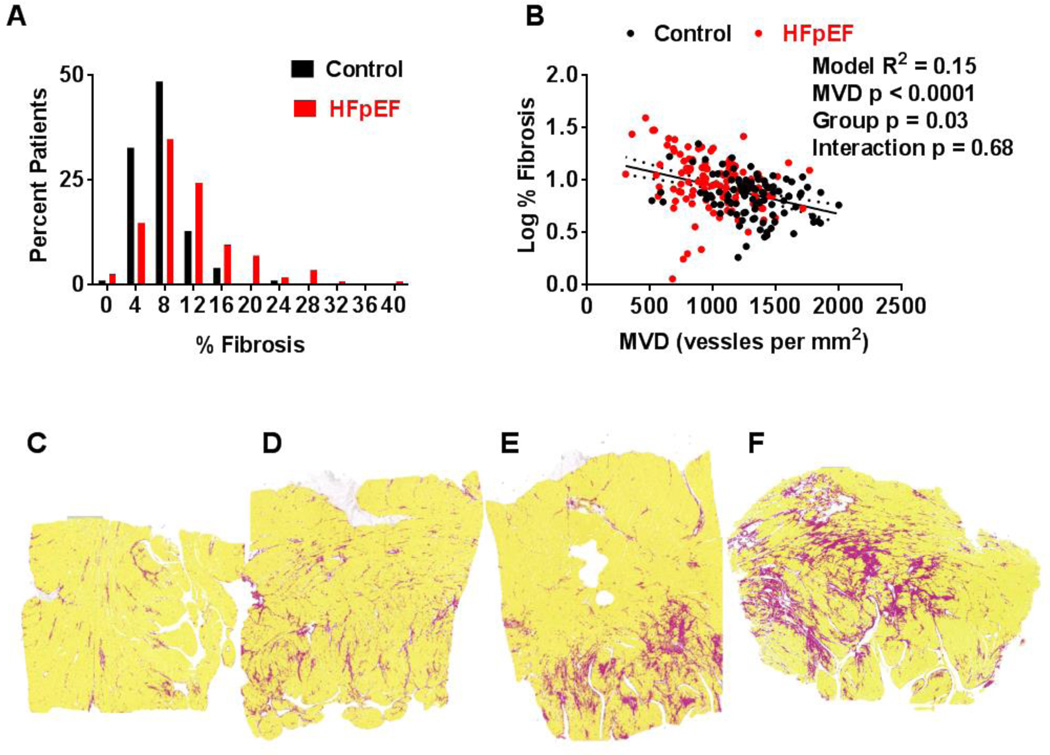
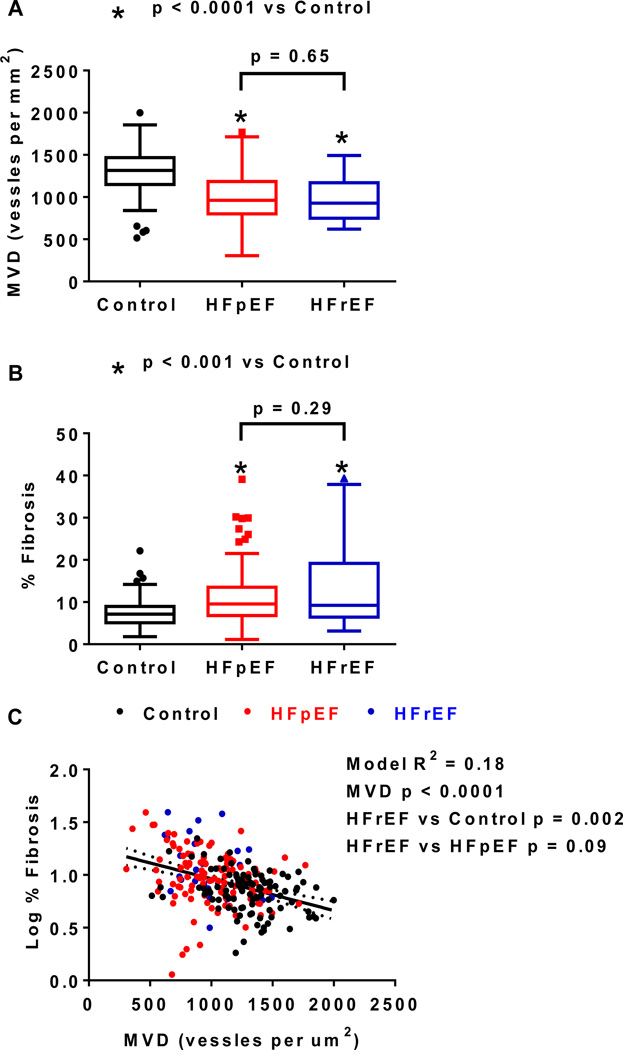
Methods and results: We identified HFpEF patients (n=124) and age-appropriate control subjects (noncardiac death, no heart failure diagnosis; n=104) who underwent autopsy. Heart weight and CAD severity were obtained from the autopsy reports. With the use of whole-field digital microscopy and automated analysis algorithms in full-thickness left ventricular sections, microvascular density (MVD), myocardial fibrosis, and their relationship were quantified. Subjects with HFpEF had heavier hearts (median, 538 g; 169% of age-, sex-, and body size-expected heart weight versus 335 g; 112% in controls), more severe CAD (65% with ≥1 vessel with >50% diameter stenosis in HFpEF versus 13% in controls), more left ventricular fibrosis (median % area fibrosis, 9.6 versus 7.1) and lower MVD (median 961 versus 1316 vessels/mm(2)) than control (P<0.0001 for all). Myocardial fibrosis increased with decreasing MVD in controls (r=-0.28, P=0.004) and HFpEF (r=-0.26, P=0.004). Adjusting for MVD attenuated the group differences in fibrosis. Heart weight, fibrosis, and MVD were similar in HFpEF patients with CAD versus without CAD.
Conclusions: In this study, patients with HFpEF had more cardiac hypertrophy, epicardial CAD, coronary microvascular rarefaction, and myocardial fibrosis than controls. Each of these findings may contribute to the left ventricular diastolic dysfunction and cardiac reserve function impairment characteristic of HFpEF.
Keywords: autopsy; endothelium; fibrosis; heart failure, diastolic; hypertrophy; microvessels; pathology.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
What the dead can teach the living: systemic nature of heart failure with preserved ejection fraction.Circulation. 2015 Feb 10;131(6):522-4. doi: 10.1161/CIRCULATIONAHA.114.014420. Epub 2014 Dec 31. Circulation. 2015. PMID: 25552355 Free PMC article. No abstract available.
-
Letter by Edwards et al Regarding Article, "Coronary Microvascular Rarefaction and Myocardial Fibrosis in Heart Failure With Preserved Ejection Fraction".Circulation. 2015 Oct 20;132(16):e204. doi: 10.1161/CIRCULATIONAHA.115.016295. Circulation. 2015. PMID: 26481570 No abstract available.
-
Letter by Campbell Regarding Article, "Coronary Microvascular Rarefaction and Myocardial Fibrosis in Heart Failure With Preserved Ejection Fraction".Circulation. 2015 Oct 20;132(16):e205. doi: 10.1161/CIRCULATIONAHA.115.016091. Circulation. 2015. PMID: 26481571 No abstract available.
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263–271. - PubMed
-
- Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure--abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–1959. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
