

Optimal achieved blood pressure in acute intracerebral hemorrhage: INTERACT2
- PMID: 25552575
- PMCID: PMC4336065
- DOI: 10.1212/WNL.0000000000001205
Optimal achieved blood pressure in acute intracerebral hemorrhage: INTERACT2
Abstract
Objectives: To investigate the effects of intensive blood pressure (BP) lowering according to baseline BP levels and optimal achieved BP levels in patients with acute intracerebral hemorrhage (ICH).
Methods: INTERACT2 was an open, blinded endpoint, randomized controlled trial in 2,839 patients with ICH within 6 hours of onset and elevated systolic BP (SBP) (150-220 mm Hg) who were allocated to receive intensive (target SBP <140 mm Hg within 1 hour, with lower limit of 130 mm Hg for treatment cessation) or guideline-recommended (target SBP <180 mm Hg) BP-lowering treatment. Outcome was physical function across all 7 levels of the modified Rankin Scale at 90 days.
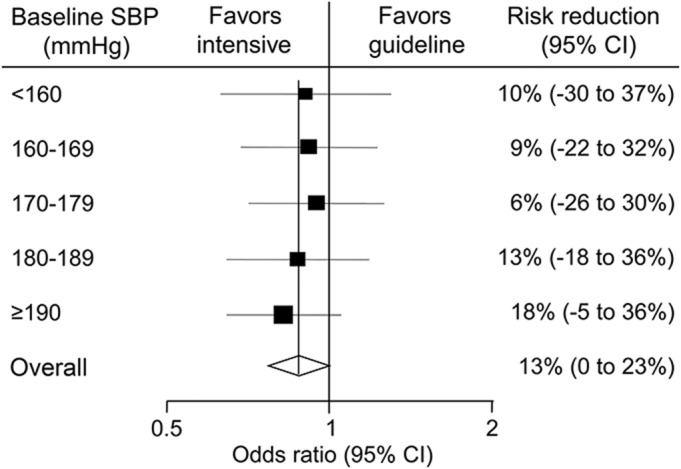
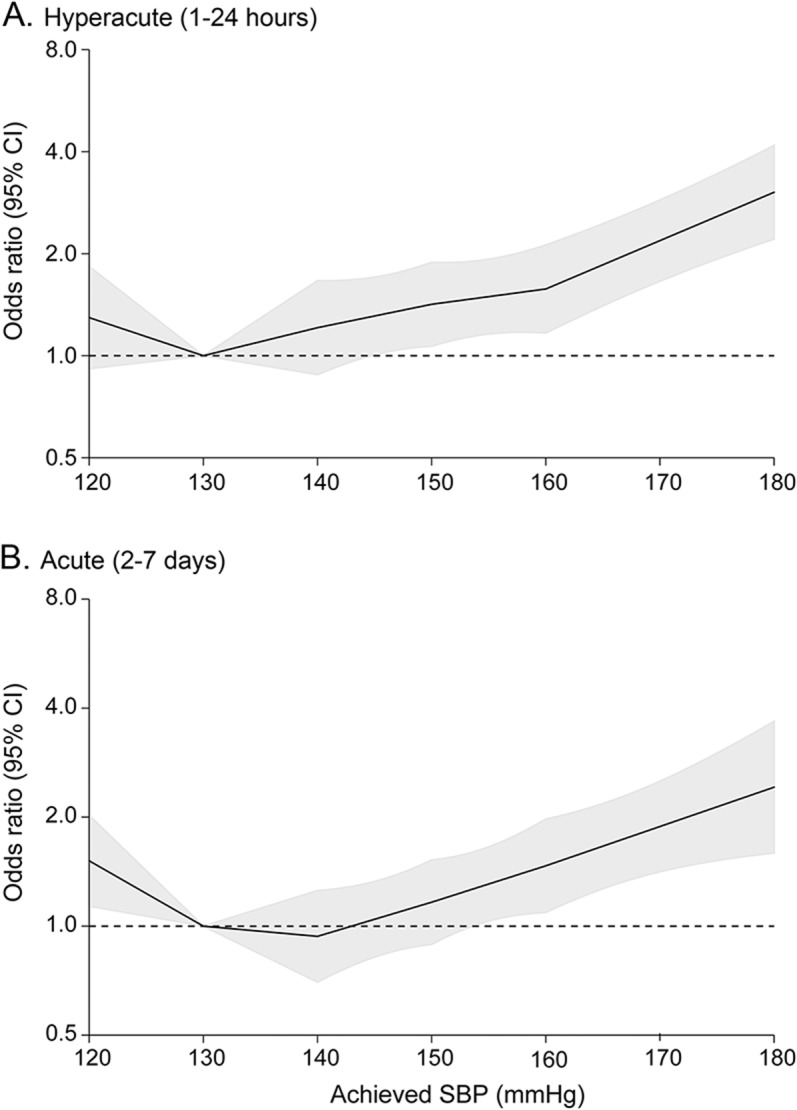
Results: Analysis of the randomized comparisons showed that intensive BP lowering produced comparable benefits on physical function at 90 days in 5 subgroups defined by baseline SBP of <160, 160-169, 170-179, 180-189, and ≥190 mm Hg (p homogeneity = 0.790). Analyses of achieved BP showed linear increases in the risk of physical dysfunction for achieved SBP above 130 mm Hg for both hyperacute (1-24 hours) and acute (2-7 days) phases while modest increases were also observed for achieved SBP below 130 mm Hg.
Conclusions: Intensive BP lowering appears beneficial across a wide range of baseline SBP levels, and target SBP level of 130-139 mm Hg is likely to provide maximum benefit in acute ICH.
Classification of evidence: This study provides Class I evidence that the effect of intensive BP lowering on physical function is not influenced by baseline BP.
© 2014 American Academy of Neurology.
Figures
Comment in
-
Seeking best medical treatment for hyperacute intracerebral hemorrhage.Neurology. 2015 Feb 3;84(5):444-5. doi: 10.1212/WNL.0000000000001221. Epub 2014 Dec 31. Neurology. 2015. PMID: 25552577 No abstract available.
-
Optimal achieved blood pressure in acute intracerebral hemorrhage: INTERACT2.Neurology. 2015 Aug 11;85(6):557-8. doi: 10.1212/01.wnl.0000470918.40985.d0. Neurology. 2015. PMID: 26259858 No abstract available.
-
Author Response.Neurology. 2015 Aug 11;85(6):558. Neurology. 2015. PMID: 26484369 No abstract available.
References
-
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, et al. ; Global Burden of Diseases, Injuries, Risk Factors Study 2010 (GBD 2010), GBD Stroke Experts Group. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet Glob Health 2013;1:e259–e281. - PMC - PubMed
-
- Liu M, Wu B, Wang WZ, Lee LM, Zhang SH, Kong LZ. Stroke in China: epidemiology, prevention, and management strategies. Lancet Neurol 2007;6:456–464. - PubMed
-
- Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortality after intracerebral hemorrhage. Neurology 2006;66:1182–1186. - PubMed
-
- Robinson TG, Potter JF. Blood pressure after stroke. Age Ageing 2004;33:6–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials