

Deciphering the molecular landscape in chronic lymphocytic leukemia: time frame of disease evolution
- PMID: 25552678
- PMCID: PMC4281307
- DOI: 10.3324/haematol.2014.115923
Deciphering the molecular landscape in chronic lymphocytic leukemia: time frame of disease evolution
Abstract
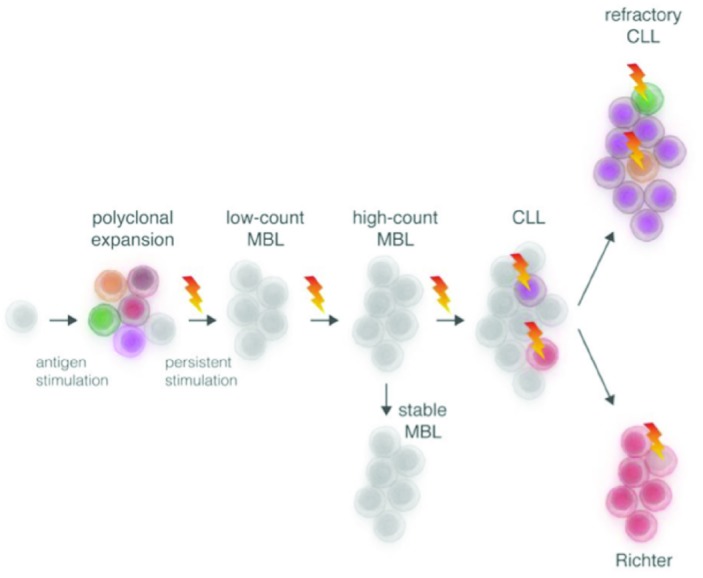
Dramatic advances in next generation sequencing technologies have provided a novel opportunity to understand the molecular genetics of chronic lymphocytic leukemia through the comprehensive detection of genetic lesions. While progress is being made in elucidating the clinical significance of recurrently mutated genes, layers of complexity have been added to our understanding of chronic lymphocytic leukemia pathogenesis in the guise of the molecular evolution and (sub)clonal architecture of the disease. As we prepare for an era of tailored therapy, we need to appreciate not only the effect mutations have on drug response but also the impact subclones containing specific mutations have at initial presentation, during therapy and upon relapse. Therefore, although the wealth of emerging genetic data has great potential in helping us devise strategies to improve the therapy and prognosis of patients, focused efforts will be required to follow disease evolution, particularly in the context of novel therapies, in order to translate this knowledge into clinical settings.
Copyright© Ferrata Storti Foundation.
Figures


References
-
- Hallek M, Cheson BD, Catovsky D, Caligaris-Cappio F, Dighiero G, Dohner H, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12): 5446–56. - PMC - PubMed
-
- Hallek M, Fischer K, Fingerle-Rowson G, Fink AM, Busch R, Mayer J, et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet. 2010;376(9747):1164–74. - PubMed
-
- Zenz T, Habe S, Denzel T, Mohr J, Winkler D, Buhler A, et al. Detailed analysis of p53 pathway defects in fludarabine-refractory chronic lymphocytic leukemia (CLL): dissecting the contribution of 17p deletion, TP53 mutation, p53-p21 dysfunction, and miR34a in a prospective clinical trial. Blood. 2009;114(13):2589–97. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
