

Diagnostic dilemma: Sturge-Weber syndrome, without facial nevus
- PMID: 25552865
- PMCID: PMC4244768
- DOI: 10.4103/0976-3147.143215
Diagnostic dilemma: Sturge-Weber syndrome, without facial nevus
Abstract
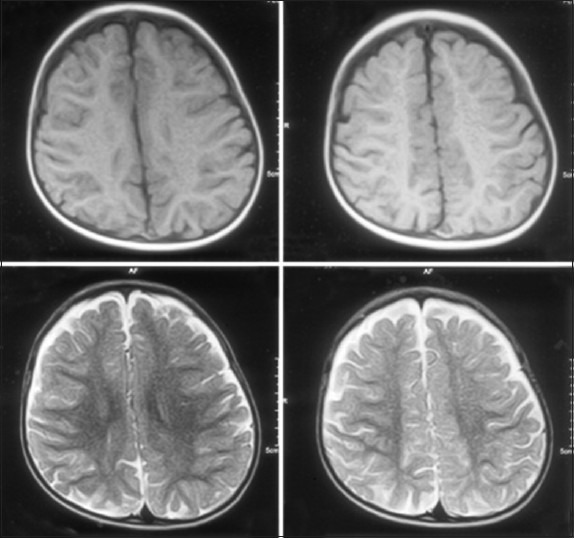
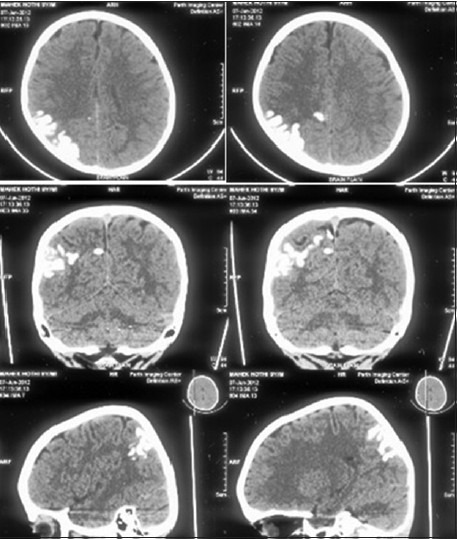
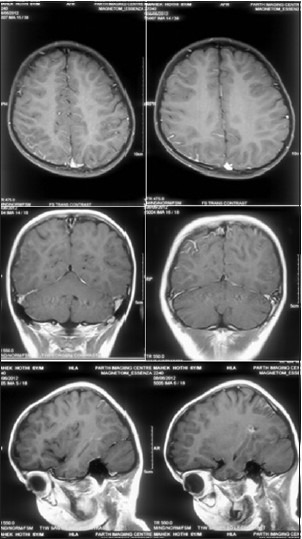
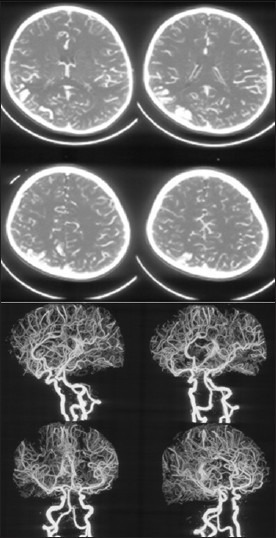
Sturge-Weber syndrome (SWS), a rare sporadic neurocutaneous disease, is characterized by a congenital unilateral port-wine nevus affecting the area innervated by V1, ipsilateral leptomeningeal angiomatosis, and calcification in the occipital or frontoparietal region and glaucoma/vascular eye abnormality. Three types of SWS have been described in literature: Type I (classic) demonstrates facial and leptomeningeal angioma, often with glaucoma; type II has facial angioma and glaucoma, with no evidence of intracranial lesions; and type III (rarest) presents with only leptomeningeal angioma. Only a few cases of type III SWS have been reported. Here, we report a case of a seven-year-old boy with focal complex partial seizure, who was diagnosed with SWS without facial nevus. Recognition of this type of SWS is important, as our patient had been misdiagnosed and received inappropriate antiepileptic drugs for six years. We suggest that in the appropriate clinical scenario, the diagnosis of SWS without facial nevus should be considered before labelling idiopathic or cryptogenic localization-related epilepsy, and gadolinium-enhanced magnetic resonance imaging (MRI) should be done in clinically suspicious cases of SWS, without facial nevus.
Keywords: Facial nevus; Sturge-Weber syndrome; gyral calcification; leptomeningeal angiomatosis.
Conflict of interest statement
Figures
References
-
- Bodensteiner JB, Roach ES, editors. SturgeWeber syndrome. Mt. Freedom, NJ: Sturge Weber Foundation; 1999. pp. 1–8.
-
- Pascual-Castroviejo I, Díaz-Gonzalez C, García-Melian RM, Gonzalez-Casado I, Muñoz-Hiraldo E. Sturge-Weber syndrome: Study of 40 patients. PediatrNeurol. 1993;9:283–8. - PubMed
-
- Roach ES. Neurocutaneous syndromes. Pediatr Clin North Am. 1992;39:591–620. - PubMed
-
- Grururaj AK, Sztriha L, Johansen J, Nork M. Sturge-Weber syndrome without facial nevus: A case report and review of the literature. Acta Paediatr. 2000;89:740–3. - PubMed
-
- Martínez-Bermejo A, Tendero A, López-Martín V, Arcas J, Royo A, Polanco I, et al. Occipital leptomeningealangiomatosis without facial angioma. Could it be considered a variant of Sturge-Weber syndrome? Rev Neurol. 2000;30:837–41. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources