

Is the World Health Organization-recommended dose of pralidoxime effective in the treatment of organophosphorus poisoning? A randomized, double-blinded and placebo-controlled trial
- PMID: 25558199
- PMCID: PMC4279350
- DOI: 10.4103/1658-354X.146306
Is the World Health Organization-recommended dose of pralidoxime effective in the treatment of organophosphorus poisoning? A randomized, double-blinded and placebo-controlled trial
Abstract
Background: Organophosphorus poisoning (OPP) is a major global public health problem. Pralidoxime has been used in a complimentary role to atropine for the management of OPP. World Health Organization (WHO) recommends use of pralidoxime but studies regarding its role have been inconclusive, ranging from being ineffective to harmful or beneficial.
Materials and methods: The present study was undertaken to evaluate the effectiveness of pralidoxime. Eddleston's study was the most compelling factor for our study, as he showed worst outcomes using pralidoxime. Our practice of continuous use of pralidoxime was based on the WHO guidelines and the study by Pawar (2006), which showed better outcome with higher doses of pralidoxime. These conflicting results suggested that a re-evaluation of its use in our clinical practice was indicated.
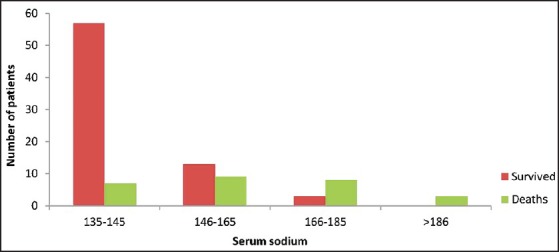
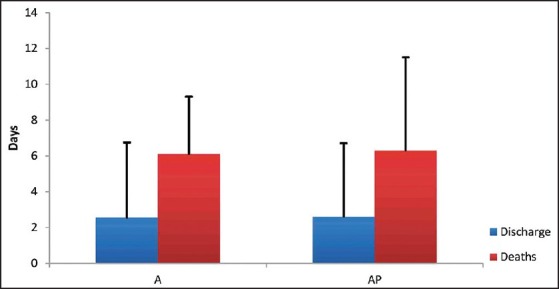
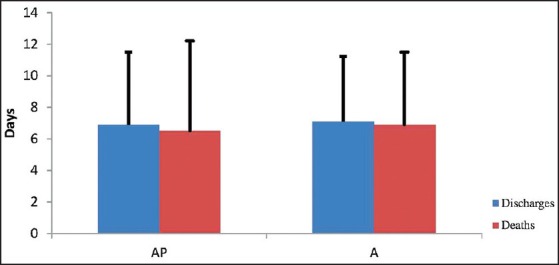
Results: There was no difference in mortality rates, hemodynamic parameters and atropine requirements between the AP and A groups. Mean duration of ventilation (3.6 ± 4.6 in AP group vs. 3.6 ± 4.4 in A group) and Intensive Care Unit stay (7.1 ± 5.4 in AP group vs. 6.8 ± 4.7 in A group) was comparable. Serum sodium concentrations showed a correlation with mortality, with lower concentrations associated with better outcomes.
Conclusion: The study suggests that add-on WHO-recommended pralidoxime therapy does not provide any benefit over atropine monotherapy. Adding pralidoxime does not seem to be beneficial and at the same time does not result in increased mortality rates. Our practice changed after completion of this study, and it has proven to be of significant benefit to patients who had to bear the expense of treatment.
Keywords: Acetyl-cholinesterase; atropine; organophosphorous poisoning; pralidoxime; pseudo-cholinesterase; ventilation.
Conflict of interest statement
Figures
References
-
- Joshi S, Biswas B, Malla G. Management of organophosphorus poisoning. Indian J Pharmacol. 2006;41:69–70.
-
- Malik GM, Mubarik M, Romshoo GJ. Organophosphorus poisoning in the Kashmir Valley, 1994 to 1997. N Engl J Med. 1998;338:1078. - PubMed
-
- Chugh SN, Agarwal N, Dabla S. Comparative evaluation of “atropine alone” and atropine with pralidoxime in the management of organophosphorus poisoning. J Indian Acad Clin Med. 2006;6:33–7.
-
- du Toit PW, Müller FO, van Tonder WM, Ungerer MJ. Experience with the intensive care management of organophosphate insecticide poisoning. S Afr Med J. 1981;60:227–9. - PubMed
-
- Pawar KS, Bhoite RR, Pillay CP, Chavan SC, Malshikare DS, Garad SG. Continuous pralidoxime infusion versus repeated bolus injection to treat organophosphorus pesticide poisoning: A randomised controlled trial. Lancet. 2006;368:2136–41. - PubMed
LinkOut - more resources
Full Text Sources
Medical
