

Effect of Medicare's nonpayment for Hospital-Acquired Conditions: lessons for future policy
- PMID: 25559166
- PMCID: PMC5508870
- DOI: 10.1001/jamainternmed.2014.5486
Effect of Medicare's nonpayment for Hospital-Acquired Conditions: lessons for future policy
Abstract
Importance: In 2008, Medicare implemented the Hospital-Acquired Conditions (HACs) Initiative, a policy denying incremental payment for 8 complications of hospital care, also known as never events. The regulation's effect on these events has not been well studied.
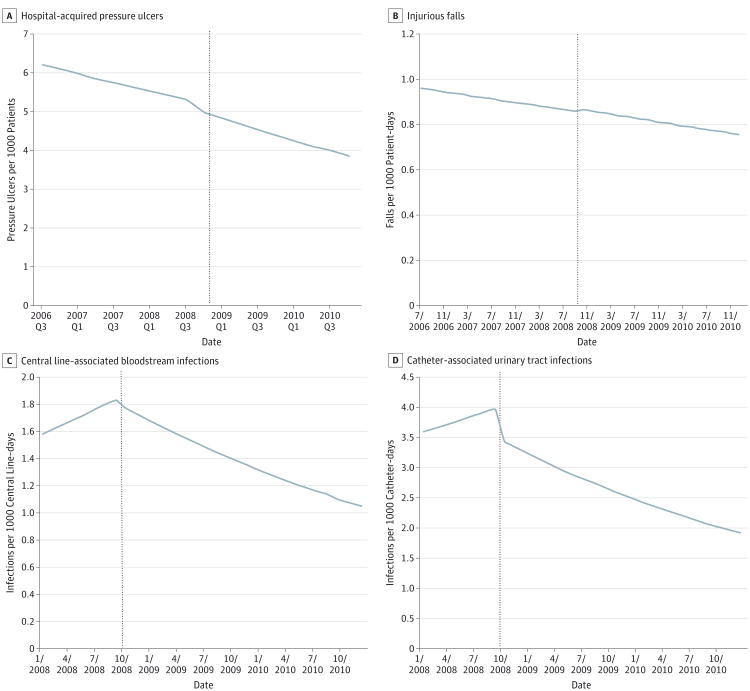
Objective: To measure the association between Medicare's nonpayment policy and 4 outcomes addressed by the HACs Initiative: central line-associated bloodstream infections (CLABSIs), catheter-associated urinary tract infections (CAUTIs), hospital-acquired pressure ulcers (HAPUs), and injurious inpatient falls.
Design, setting, and participants: Quasi-experimental study of adult nursing units from 1381 US hospitals participating in the National Database of Nursing Quality Indicators (NDNQI), a program of the American Nurses Association. The NDNQI data were combined with American Hospital Association, Medicare Cost Report, and local market data to examine adjusted outcomes. Multilevel models were used to evaluate the effect of Medicare's nonpayment policy on never events.
Exposures: United States hospitals providing treatment for Medicare patients were subject to the new payment policy beginning in October 2008.
Main outcomes and measures: Changes in unit-level rates of HAPUs, injurious falls, CLABSIs, and CAUTIs after initiation of the policy.
Results: Medicare's nonpayment policy was associated with an 11% reduction in the rate of change in CLABSIs (incidence rate ratio [IRR], 0.89; 95% CI, 0.83-0.95) and a 10% reduction in the rate of change in CAUTIs (IRR, 0.90; 95% CI, 0.85-0.95), but was not associated with a significant change in injurious falls (IRR, 0.99; 95% CI, 0.99-1.00) or HAPUs (odds ratio, 0.98; 95% CI, 0.96-1.01). Consideration of unit-, hospital-, and market-level factors did not significantly alter our findings.
Conclusions and relevance: The HACs Initiative was associated with improvements in CLABSI and CAUTI trends, conditions for which there is strong evidence that better hospital processes yield better outcomes. However, the HACs Initiative was not associated with improvements in HAPU or injurious fall trends, conditions for which there is less evidence that changing hospital processes leads to significantly better outcomes.
Figures
Comment in
-
Incentivizing "structures" over "outcomes" to bridge the knowing-doing gap.JAMA Intern Med. 2015 Mar;175(3):354-5. doi: 10.1001/jamainternmed.2014.5293. JAMA Intern Med. 2015. PMID: 25561391 No abstract available.
-
Ongoing Attention to Injurious Inpatient Falls and Pressure Ulcers.JAMA Intern Med. 2015 Sep;175(9):1580-1. doi: 10.1001/jamainternmed.2015.2549. JAMA Intern Med. 2015. PMID: 26348514 No abstract available.
-
Ongoing Attention to Injurious Inpatient Falls and Pressure Ulcers.JAMA Intern Med. 2015 Sep;175(9):1581-2. doi: 10.1001/jamainternmed.2015.2552. JAMA Intern Med. 2015. PMID: 26348515 No abstract available.
-
Ongoing Attention to Injurious Inpatient Falls and Pressure Ulcers--Reply.JAMA Intern Med. 2015 Sep;175(9):1582. doi: 10.1001/jamainternmed.2015.2568. JAMA Intern Med. 2015. PMID: 26348517 No abstract available.
References
-
- Centers for Medicare & Medicaid Services (CMS), HHS. Medicare program: changes to the hospital inpatient prospective payment systems and fiscal year 2008 rates. Fed Regist. 2007;72(162):47129–48175. - PubMed
-
- Rosenthal MB. Nonpayment for performance? Medicare's new reimbursement rule. N Engl J Med. 2007;357(16):1573–1575. - PubMed
-
- McNair PD, Luft HS, Bindman AB. Medicare's policy not to pay for treating hospital-acquired conditions: the impact. Health Aff (Millwood) 2009;28(5):1485–1493. - PubMed
-
- McHugh M, Martin TC, Orwat J, Dyke KV. Medicare's policy to limit payment for hospital-acquired conditions: the impact on safety net providers. J Health Care Poor Underserved. 2011;22(2):638–647. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
