

Association between dietary whole grain intake and risk of mortality: two large prospective studies in US men and women
- PMID: 25559238
- PMCID: PMC4429593
- DOI: 10.1001/jamainternmed.2014.6283
Association between dietary whole grain intake and risk of mortality: two large prospective studies in US men and women
Abstract
Importance: Higher intake of whole grains has been associated with a lower risk of major chronic diseases, such as type 2 diabetes mellitus and cardiovascular disease (CVD), although limited prospective evidence exists regarding whole grains' association with mortality.
Objective: To examine the association between dietary whole grain consumption and risk of mortality.
Design, setting, and participants: We investigated 74 341 women from the Nurses' Health Study (1984-2010) and 43 744 men from the Health Professionals Follow-Up Study (1986-2010), 2 large prospective cohort studies. All patients were free of CVD and cancer at baseline.
Main outcomes and measures: Hazard ratios (HRs) for total mortality and mortality due to CVD and cancer according to quintiles of whole grain consumption, which was updated every 2 or 4 years by using validated food frequency questionnaires.
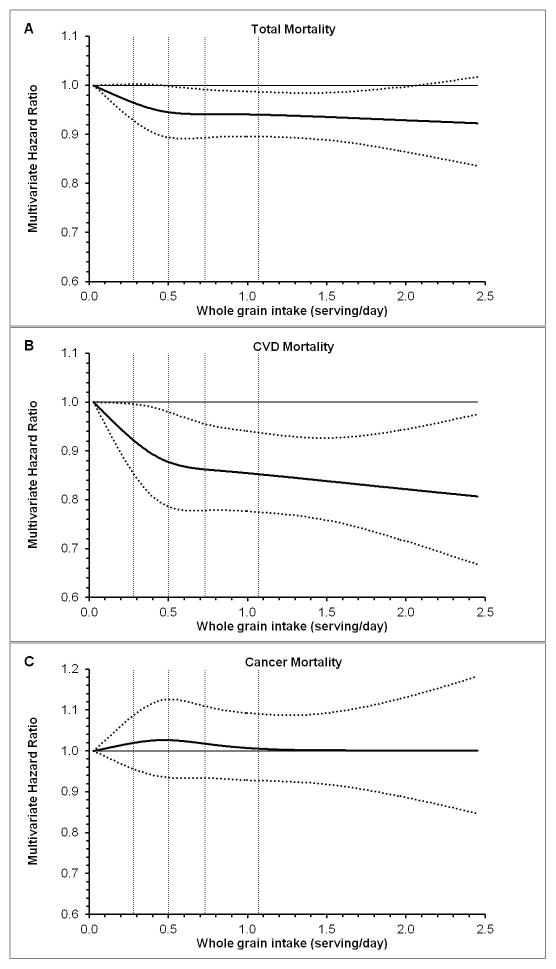
Results: We documented 26 920 deaths during 2 727 006 person-years of follow-up. After multivariate adjustment for potential confounders, including age, smoking, body mass index, physical activity, and modified Alternate Healthy Eating Index score, higher whole grain intake was associated with lower total and CVD mortality but not cancer mortality: the pooled HRs for quintiles 1 through 5, respectively, of whole grain intake were 1 (reference), 0.99 (95% CI, 0.95-1.02), 0.98 (95% CI, 0.95-1.02), 0.97 (95% CI, 0.93-1.01), and 0.91 (95% CI, 0.88-0.95) for total mortality (P fortrend < .001); 1 (reference), 0.94 (95% CI, 0.88-1.01), 0.94 (95% CI, 0.87-1.01), 0.87 (95% CI, 0.80-0.94), and 0.85 (95% CI, 0.78-0.92) for CVD mortality (P fortrend < .001); and 1 (reference), 1.02 (95% CI, 0.96-1.08), 1.05 (95% CI, 0.99-1.12), 1.04 (95% CI, 0.98-1.11), and 0.97 (95% CI, 0.91-1.04) for cancer mortality (P fortrend = .43). We further estimated that every serving (28 g/d) of whole grain consumption was associated with a 5% (95% CI, 2%-7%) lower total morality or a 9% (95% CI, 4%-13%) lower CVD mortality, whereas the same intake level was nonsignificantly associated with lower cancer mortality (HR, 0.98; 95% CI, 0.94-1.02). Similar inverse associations were observed between bran intake and CVD mortality, with a pooled HR of 0.80 (95% CI, 0.73-0.87; P fortrend < .001), whereas germ intake was not associated with CVD mortality after adjustment for bran intake.
Conclusions and relevance: These data indicate that higher whole grain consumption is associated with lower total and CVD mortality in US men and women, independent of other dietary and lifestyle factors. These results are in line with recommendations that promote increased whole grain consumption to facilitate disease prevention.
Figures
References
-
- European Food Information Council (EUFIC) [accessed November 2013];Whole grain fact sheet. http://www.eufic.org/article/en/page/BARCHIVE/expid/Whole-grain-Fact-Sheet.
-
- The Department of Agriculture (USDA) and the Department of Health and Human Services (HHS) [accessed November 2013];Dietary Guidelines for Americans. http://www.choosemyplate.gov/dietary-guidelines.html.
-
- McCarty MF. Magnesium may mediate the favorable impact of whole grains on insulin sensitivity by acting as a mild calcium antagonist. Med Hypotheses. 2005;64(3):619–627. - PubMed
-
- Juntunen KS, Niskanen LK, Liukkonen KH, et al. Postprandial glucose, insulin, and incretin responses to grain products in healthy subjects. Am J Clin Nutr. 2002;75(2):254–262. - PubMed
-
- Pereira MA, Jacobs DR, Pins JJ, et al. Effect of whole grains on insulin sensitivity in overweight hyperinsulinemic adults. Am J Clin Nutr. 2002;75(5):848–855. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 DK058845/DK/NIDDK NIH HHS/United States
- P01 CA087969/CA/NCI NIH HHS/United States
- R00HL098459/HL/NHLBI NIH HHS/United States
- P01 CA055075/CA/NCI NIH HHS/United States
- R00 HL098459/HL/NHLBI NIH HHS/United States
- R01 HL35464/HL/NHLBI NIH HHS/United States
- U19 CA055075/CA/NCI NIH HHS/United States
- U54 CA155626/CA/NCI NIH HHS/United States
- P01 CA87969/CA/NCI NIH HHS/United States
- R01 HL034594/HL/NHLBI NIH HHS/United States
- UM1 CA186107/CA/NCI NIH HHS/United States
- UM1 CA167552/CA/NCI NIH HHS/United States
- R01 DK58845/DK/NIDDK NIH HHS/United States
- R01 HL035464/HL/NHLBI NIH HHS/United States
- CA055075/CA/NCI NIH HHS/United States
- R01 HL060712/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
