

Clinical pharmacokinetics and pharmacodynamics of clopidogrel
- PMID: 25559342
- PMCID: PMC5677184
- DOI: 10.1007/s40262-014-0230-6
Clinical pharmacokinetics and pharmacodynamics of clopidogrel
Abstract
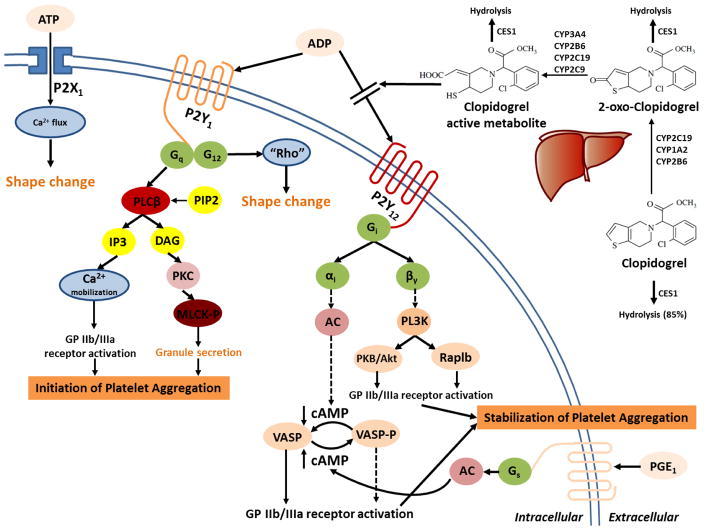
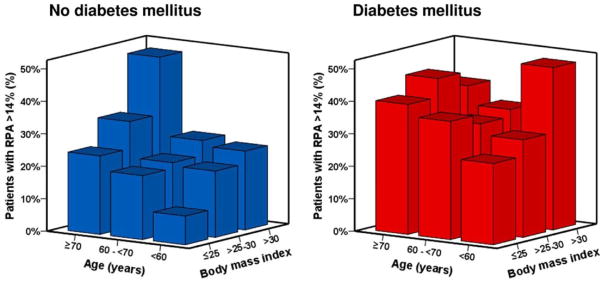
Acute coronary syndromes (ACS) remain life-threatening disorders, which are associated with high morbidity and mortality. Dual antiplatelet therapy with aspirin and clopidogrel has been shown to reduce cardiovascular events in patients with ACS. However, there is substantial inter-individual variability in the response to clopidogrel treatment, in addition to prolonged recovery of platelet reactivity as a result of irreversible binding to P2Y12 receptors. This high inter-individual variability in treatment response has primarily been associated with genetic polymorphisms in the genes encoding for cytochrome (CYP) 2C19, which affect the pharmacokinetics of clopidogrel. While the US Food and Drug Administration has issued a boxed warning for CYP2C19 poor metabolizers because of potentially reduced efficacy in these patients, results from multivariate analyses suggest that additional factors, including age, sex, obesity, concurrent diseases and drug-drug interactions, may all contribute to the overall between-subject variability in treatment response. However, the extent to which each of these factors contributes to the overall variability, and how they are interrelated, is currently unclear. The objective of this review article is to provide a comprehensive update on the different factors that influence the pharmacokinetics and pharmacodynamics of clopidogrel and how they mechanistically contribute to inter-individual differences in the response to clopidogrel treatment.
Figures
References
-
- Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2011 Dec;32(23):2999–3054. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, et al. Executive summary: heart disease and stroke statistics--2012 update: a report from the American Heart Association. Circulation. 2012 Jan 3;125(1):188–97. - PubMed
-
- Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, Alfonso F, Macaya C, Bass TA, et al. Variability in individual responsiveness to clopidogrel: clinical implications, management, and future perspectives. J Am Coll Cardiol. 2007 Apr 10;49(14):1505–16. - PubMed
-
- Boggon R, van Staa TP, Timmis A, Hemingway H, Ray KK, Begg A, et al. Clopidogrel discontinuation after acute coronary syndromes: frequency, predictors and associations with death and myocardial infarction--a hospital registry-primary care linked cohort (MINAP-GPRD) Eur Heart J. 2011 Oct;32(19):2376–86. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
