

Morbidity and survival probability in burn patients in modern burn care
- PMID: 25559438
- PMCID: PMC4359665
- DOI: 10.1097/CCM.0000000000000790
Morbidity and survival probability in burn patients in modern burn care
Abstract
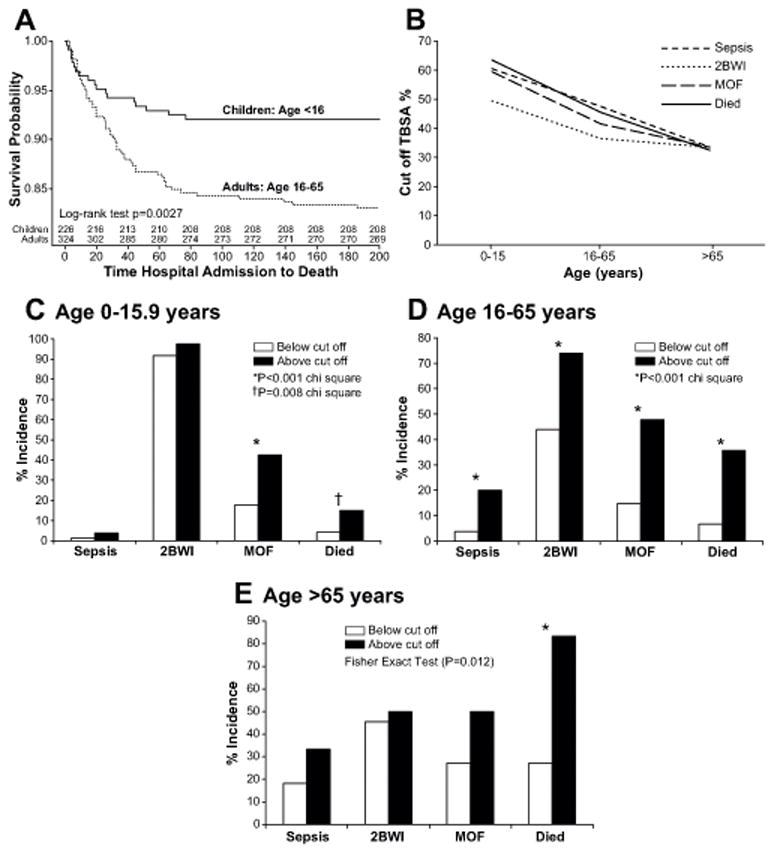
Objective: Characterizing burn sizes that are associated with an increased risk of mortality and morbidity is critical because it would allow identifying patients who might derive the greatest benefit from individualized, experimental, or innovative therapies. Although scores have been established to predict mortality, few data addressing other outcomes exist. The objective of this study was to determine burn sizes that are associated with increased mortality and morbidity after burn.
Design and patients: Burn patients were prospectively enrolled as part of the multicenter prospective cohort study, Inflammation and the Host Response to Injury Glue Grant, with the following inclusion criteria: 0-99 years old, admission within 96 hours after injury, and more than 20% total body surface area burns requiring at least one surgical intervention.
Setting: Six major burn centers in North America.
Measurements and main results: Burn size cutoff values were determined for mortality, burn wound infection (at least two infections), sepsis (as defined by American Burn Association sepsis criteria), pneumonia, acute respiratory distress syndrome, and multiple organ failure (Denver 2 score>3) for both children (<16 yr) and adults (16-65 yr). Five hundred seventy-three patients were enrolled, of which 226 patients were children. Twenty-three patients were older than 65 years and were excluded from the cutoff analysis. In children, the cutoff burn size for mortality, sepsis, infection, and multiple organ failure was approximately 60% total body surface area burned. In adults, the cutoff for these outcomes was lower, at approximately 40% total body surface area burned.
Conclusions: In the modern burn care setting, adults with over 40% total body surface area burned and children with over 60% total body surface area burned are at high risk for morbidity and mortality, even in highly specialized centers.
Conflict of interest statement
Figures
Comment in
-
Can we really predict morbidity and mortality in burn patients?Crit Care Med. 2015 Apr;43(4):918-9. doi: 10.1097/CCM.0000000000000842. Crit Care Med. 2015. PMID: 25768358 No abstract available.
References
-
- Hussain A, Choukairi F, Dunn K. Predicting survival in thermal injury: A systematic review of methodology of composite prediction models. Burns. 2013 Feb 2; Epub ahead of print. - PubMed
-
- Roberts G, Lloyd M, Parker M, et al. The Baux score is dead. Long live the Baux score: a 27-year retrospective cohort study of mortality at a regional burns service. J Trauma Acute Care Surg. 2012;72:251–256. - PubMed
-
- Choiniere M, Dumont M, Papillon J, et al. Prediction of death in patients with burns. Lancet. 1999;353:2211–2212. - PubMed
-
- Germann G, Barthold U, Lefering R, et al. The impact of risk factors and pre-existing conditions on the mortality of burn patients and the precision of predictive admission-scoring systems. Burns. 1997;23:195–203. - PubMed
Publication types
MeSH terms
Grants and funding
- U54 GM062119/GM/NIGMS NIH HHS/United States
- T32 GM0008256/GM/NIGMS NIH HHS/United States
- R24 GM102656/GM/NIGMS NIH HHS/United States
- UL1TR000071/TR/NCATS NIH HHS/United States
- KL2 RR029875/RR/NCRR NIH HHS/United States
- KL2RR029875/RR/NCRR NIH HHS/United States
- UL1 TR000071/TR/NCATS NIH HHS/United States
- U54 GM62119/GM/NIGMS NIH HHS/United States
- R01 GM056687/GM/NIGMS NIH HHS/United States
- P50 GM060338/GM/NIGMS NIH HHS/United States
- T32 GM008256/GM/NIGMS NIH HHS/United States
- 123336/Canadian Institutes of Health Research/Canada
- R01 GM087285/GM/NIGMS NIH HHS/United States
- UL1 RR029876/RR/NCRR NIH HHS/United States
- UL1RR029876/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
