

Differences in vital signs between elderly and nonelderly patients prior to ward cardiac arrest
- PMID: 25559439
- PMCID: PMC4359655
- DOI: 10.1097/CCM.0000000000000818
Differences in vital signs between elderly and nonelderly patients prior to ward cardiac arrest
Abstract
Objectives: Vital signs and composite scores, such as the Modified Early Warning Score, are used to identify high-risk ward patients and trigger rapid response teams. Although age-related vital sign changes are known to occur, little is known about the differences in vital signs between elderly and nonelderly patients prior to ward cardiac arrest. We aimed to compare the accuracy of vital signs for detecting cardiac arrest between elderly and nonelderly patients.
Design: Observational cohort study.
Setting: Five hospitals in the United States.
Patients: A total of 269,956 patient admissions to the wards with documented age, including 422 index ward cardiac arrests.
Interventions: None.
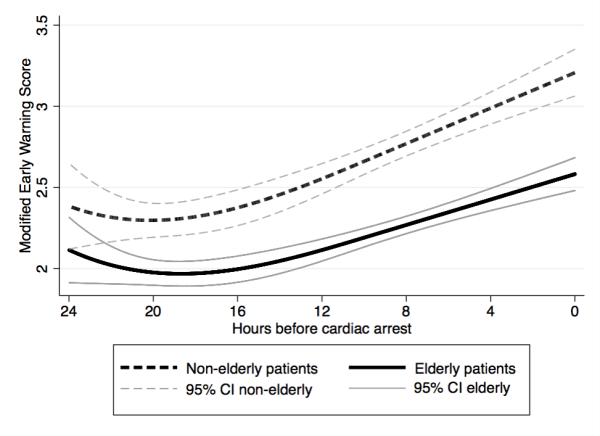
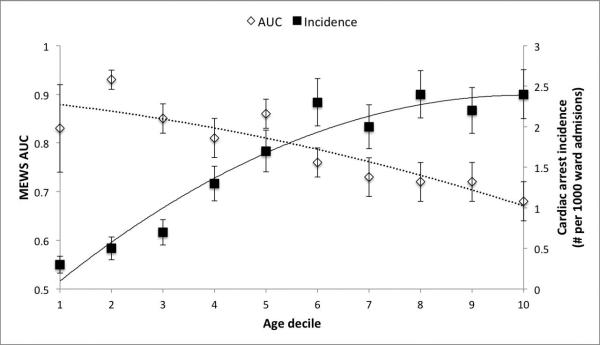
Measurements and main results: Patient characteristics and vital signs prior to cardiac arrest were compared between elderly (age, 65 yr or older) and nonelderly (age, <65 yr) patients. The area under the receiver operating characteristic curve for vital signs and the Modified Early Warning Score were also compared. Elderly patients had a higher cardiac arrest rate (2.2 vs 1.0 per 1,000 ward admissions; p<0.001) and in-hospital mortality (2.9% vs 0.7%; p<0.001) than nonelderly patients. Within 4 hours of cardiac arrest, elderly patients had significantly lower mean heart rate (88 vs 99 beats/min; p<0.001), diastolic blood pressure (60 vs 66 mm Hg; p=0.007), shock index (0.82 vs 0.93; p<0.001), and Modified Early Warning Score (2.6 vs 3.3; p<0.001) and higher pulse pressure index (0.45 vs 0.41; p<0.001) and temperature (36.4°C vs 36.3°C; p=0.047). The area under the receiver operating characteristic curves for all vital signs and the Modified Early Warning Score were higher for nonelderly patients than elderly patients (Modified Early Warning Score area under the receiver operating characteristic curve 0.85 [95% CI, 0.82-0.88] vs 0.71 [95% CI, 0.68-0.75]; p<0.001).
Conclusions: Vital signs more accurately detect cardiac arrest in nonelderly patients compared with elderly patients, which has important implications for how they are used for identifying critically ill patients. More accurate methods for risk stratification of elderly patients are necessary to decrease the occurrence of this devastating event.
Figures
Similar articles
-
Derivation of a cardiac arrest prediction model using ward vital signs*.Crit Care Med. 2012 Jul;40(7):2102-8. doi: 10.1097/CCM.0b013e318250aa5a. Crit Care Med. 2012. PMID: 22584764 Free PMC article.
-
Validation of Early Warning Scores at Two Long-Term Acute Care Hospitals.Crit Care Med. 2019 Dec;47(12):e962-e965. doi: 10.1097/CCM.0000000000004026. Crit Care Med. 2019. PMID: 31567342 Free PMC article.
-
The value of vital sign trends for detecting clinical deterioration on the wards.Resuscitation. 2016 May;102:1-5. doi: 10.1016/j.resuscitation.2016.02.005. Epub 2016 Feb 16. Resuscitation. 2016. PMID: 26898412 Free PMC article.
-
Risk stratification of hospitalized patients on the wards.Chest. 2013 Jun;143(6):1758-1765. doi: 10.1378/chest.12-1605. Chest. 2013. PMID: 23732586 Free PMC article. Review.
-
Postoperative ward monitoring - Why and what now?Best Pract Res Clin Anaesthesiol. 2019 Jun;33(2):229-245. doi: 10.1016/j.bpa.2019.06.005. Epub 2019 Jul 23. Best Pract Res Clin Anaesthesiol. 2019. PMID: 31582102 Review.
Cited by
-
Risk factors for cardiopulmonary and respiratory arrest in medical and surgical hospital patients on opioid analgesics and sedatives.PLoS One. 2018 Mar 22;13(3):e0194553. doi: 10.1371/journal.pone.0194553. eCollection 2018. PLoS One. 2018. PMID: 29566020 Free PMC article.
-
Exploring the impact of age on the predictive power of the National Early Warning score (NEWS) 2, and long-term prognosis among patients reviewed by a Rapid Response Team: A prospective, multi-centre study.Resusc Plus. 2024 Dec 10;21:100839. doi: 10.1016/j.resplu.2024.100839. eCollection 2025 Jan. Resusc Plus. 2024. PMID: 39811470 Free PMC article.
-
Association between intensive care unit transfer delay and hospital mortality: A multicenter investigation.J Hosp Med. 2016 Nov;11(11):757-762. doi: 10.1002/jhm.2630. Epub 2016 Jun 28. J Hosp Med. 2016. PMID: 27352032 Free PMC article.
-
Eleven years of experience in operating a pediatric rapid response system at a children's hospital in South Korea.Acute Crit Care. 2023 Nov;38(4):498-506. doi: 10.4266/acc.2023.01354. Epub 2023 Nov 29. Acute Crit Care. 2023. PMID: 38052515 Free PMC article.
-
Early warning scores and trigger recommendations must be used with care in older home nursing care patients: Results from an observational study.Nurs Open. 2023 Jul;10(7):4737-4746. doi: 10.1002/nop2.1724. Epub 2023 Mar 14. Nurs Open. 2023. PMID: 36916829 Free PMC article.
References
-
- Smith AF, Wood J. Can some in-hospital cardio-respiratory arrests be prevented? A prospective survey. Resuscitation. 1998;37(3):133–7. - PubMed
-
- Hodgetts TJ, Kenward G, Vlackonikolis I, Payne S, Castle N, Crouch R, et al. Incidence, location and reasons for avoidable in-hospital cardiac arrest in a district general hospital. Resuscitation. 2002;54(2):115–23. - PubMed
-
- Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. QJM. 2001;94(10):521–6. - PubMed
-
- Chan PS, Khalid A, Longmore LS, Berg RA, Kosiborod M, Spertus JA. Hospital-wide code rates and mortality before and after implementation of a rapid response team. JAMA. 2008;300(21):2506–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
