

Mesh sacrocolpopexy compared with native tissue vaginal repair: a systematic review and meta-analysis
- PMID: 25560102
- PMCID: PMC4352548
- DOI: 10.1097/AOG.0000000000000570
Mesh sacrocolpopexy compared with native tissue vaginal repair: a systematic review and meta-analysis
Abstract
Objective: To systematically review outcomes after mesh sacrocolpopexy compared with native tissue vaginal repairs in women with apical prolapse.
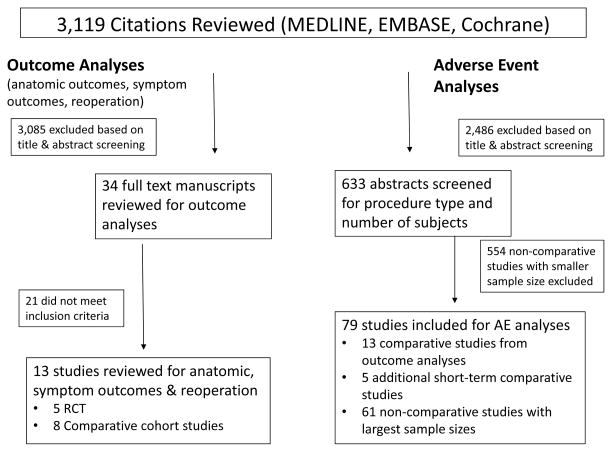
Data sources: We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov through June 4, 2012.
Methods of study selection: For anatomic and functional analyses, we included studies comparing mesh sacrocolpopexy to native tissue vaginal repairs with at least 6 months follow-up. The primary outcome was anatomic "success" after surgery. Secondary outcomes were reoperation and symptom outcomes. We included large case series and comparative studies with shorter follow-up to increase power for adverse event analyses.
Tabulation, integration, and results: Evidence quality was assessed with the Grades for Recommendation, Assessment, Development and Evaluation system. Meta-analyses were performed when at least three studies reported the same outcome. We included 13 comparative studies for anatomic success, reoperation, and symptom outcomes. Moderate-quality evidence supports improved anatomic outcomes after mesh sacrocolpopexy; very low-quality evidence shows no differences in reoperation between sacrocolpopexy and native tissue vaginal repairs. Evidence was insufficient regarding which procedures result in improved bladder or bowel symptoms. Low-quality evidence showed no differences in postoperative sexual function. Adverse event data were compiled and meta-analyzed from 79 studies. When including larger noncomparative studies, ileus or small bowel obstruction (2.7% compared with 0.2%, P<.01), mesh or suture complications (4.2% compared with 0.4%, P<.01), and thromboembolic phenomena (0.6% compared with 0.1%, P=.03) were more common after mesh sacrocolpopexy compared with native tissue vaginal repairs.
Conclusion: When anatomic durability is a priority, we suggest that mesh sacrocolpopexy may be the preferred surgical option. When minimizing adverse events or reoperation is the priority, there is no strong evidence supporting one approach over the other.
Figures



References
-
- Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 2010 Jan;21(1):5–26. - PubMed
-
- Rooney K, Kenton K, Mueller ER, FitzGerald MP, Brubaker L. Advanced anterior vaginal wall prolapse is highly correlated with apical prolapse. Am J Obstet Gynecol. 2006 Dec;195(6):1837–40. - PubMed
-
- Brubaker L, Bump RC, Fynes M. In: Abrams P, Cordozo L, Koury S, Wein A, editors. Surgery for pelvic organ prolapse; 3rd International Consultation on Incontinence; Paris: Health Publication Ltd; 2005.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
