

Effect of open-label infusion of an apoA-I-containing particle (CER-001) on RCT and artery wall thickness in patients with FHA
- PMID: 25561459
- PMCID: PMC4340317
- DOI: 10.1194/jlr.M055665
Effect of open-label infusion of an apoA-I-containing particle (CER-001) on RCT and artery wall thickness in patients with FHA
Abstract
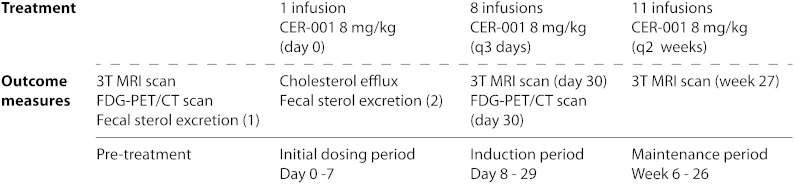
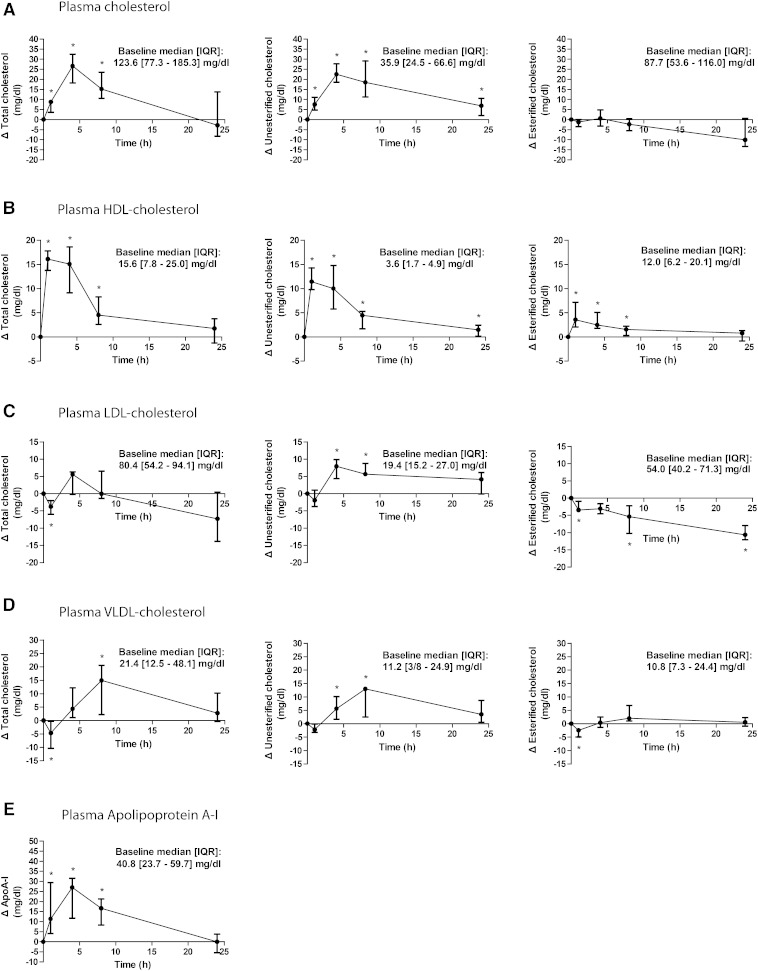
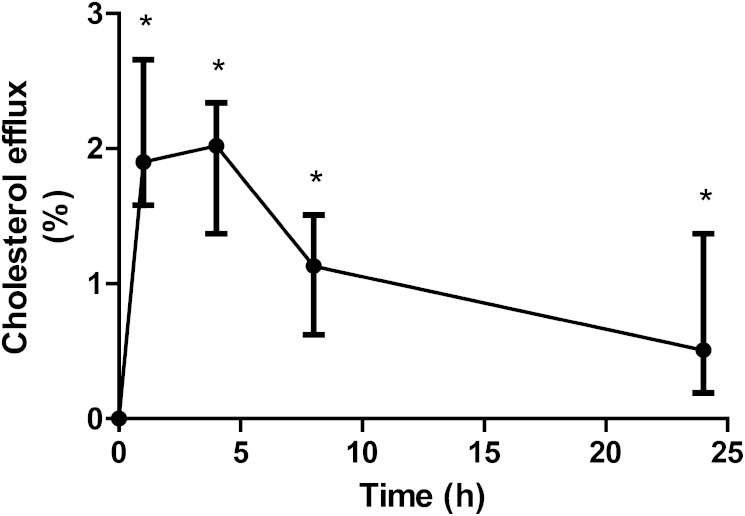
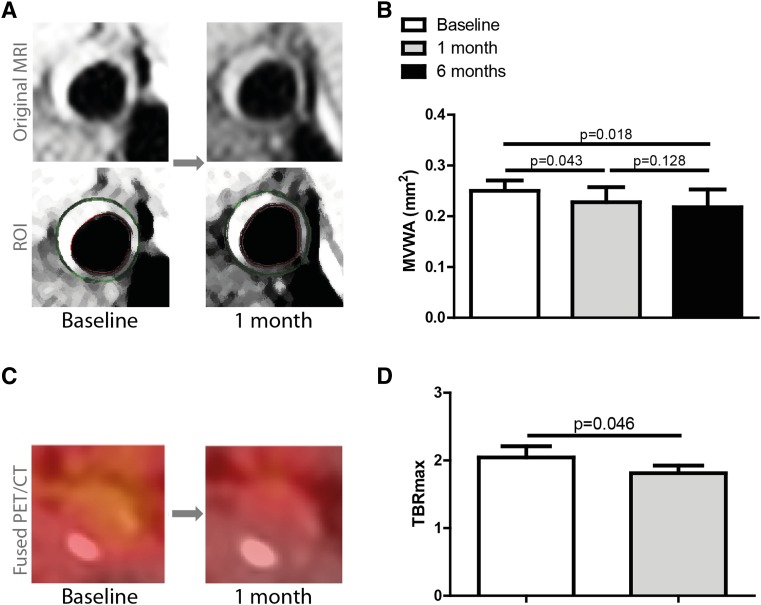
Reverse cholesterol transport (RCT) contributes to the anti-atherogenic effects of HDL. Patients with the orphan disease, familial hypoalphalipoproteinemia (FHA), are characterized by decreased tissue cholesterol removal and an increased atherogenic burden. We performed an open-label uncontrolled proof-of-concept study to evaluate the effect of infusions with a human apoA-I-containing HDL-mimetic particle (CER-001) on RCT and the arterial vessel wall in FHA. Subjects received 20 infusions of CER-001 (8 mg/kg) during 6 months. Efficacy was assessed by measuring (apo)lipoproteins, plasma-mediated cellular cholesterol efflux, fecal sterol excretion (FSE), and carotid artery wall dimension by MRI and artery wall inflammation by (18)F-fluorodeoxyglucose-positron emission tomography/computed tomography scans. We included seven FHA patients: HDL-cholesterol (HDL-c), 13.8 [1.8-29.1] mg/dl; apoA-I, 28.7 [7.9-59.1] mg/dl. Following nine infusions in 1 month, apoA-I and HDL-c increased directly after infusion by 27.0 and 16.1 mg/dl (P = 0.018). CER-001 induced a 44% relative increase (P = 0.018) in in vitro cellular cholesterol efflux with a trend toward increased FSE (P = 0.068). After nine infusions of CER-001, carotid mean vessel wall area decreased compared with baseline from 25.0 to 22.8 mm(2) (P = 0.043) and target-to-background ratio from 2.04 to 1.81 (P = 0.046). In FHA-subjects, CER-001 stimulates cholesterol mobilization and reduces artery wall dimension and inflammation, supporting further evaluation of CER-001 in FHA patients.
Keywords: apolipoprotein A-I; familial hypoalphalipoproteinemia; reverse cholesterol transport.
Copyright © 2015 by the American Society for Biochemistry and Molecular Biology, Inc.
Figures
References
-
- Kannel W. B., Castelli W. P., Gordon T. 1979. Cholesterol in the prediction of atherosclerotic disease. New perspectives based on the Framingham study. Ann. Intern. Med. 90: 85–91. - PubMed
-
- Schwartz G. G., Olsson A. G., Abt M., Ballantyne C. M., Barter P. J., Brumm J., Chaitman B. R., Holme I. M., Kallend D., Leiter L. A., et al. 2012. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N. Engl. J. Med. 367: 2089–2099. - PubMed
-
- Boden W. E., Probstfield J. L., Anderson T., Chaitman B. R., Desvignes-Nickens P., Koprowicz K., McBride R., Teo K., Weintraub W. 2011. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N. Engl. J. Med. 365: 2255–2267. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
