

Contrast-enhanced ultrasound in portal venous system aneurysms: a multi-center study
- PMID: 25561805
- PMCID: PMC4277975
- DOI: 10.3748/wjg.v20.i48.18375
Contrast-enhanced ultrasound in portal venous system aneurysms: a multi-center study
Abstract
Aim: To investigate contrast-enhanced ultrasound (CEUS) findings in portal venous system aneurysms (PVSAs).
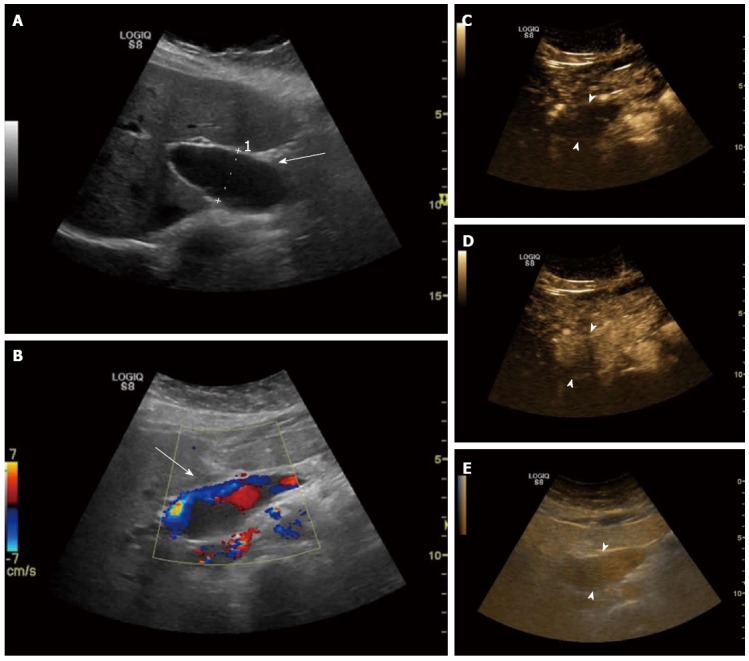
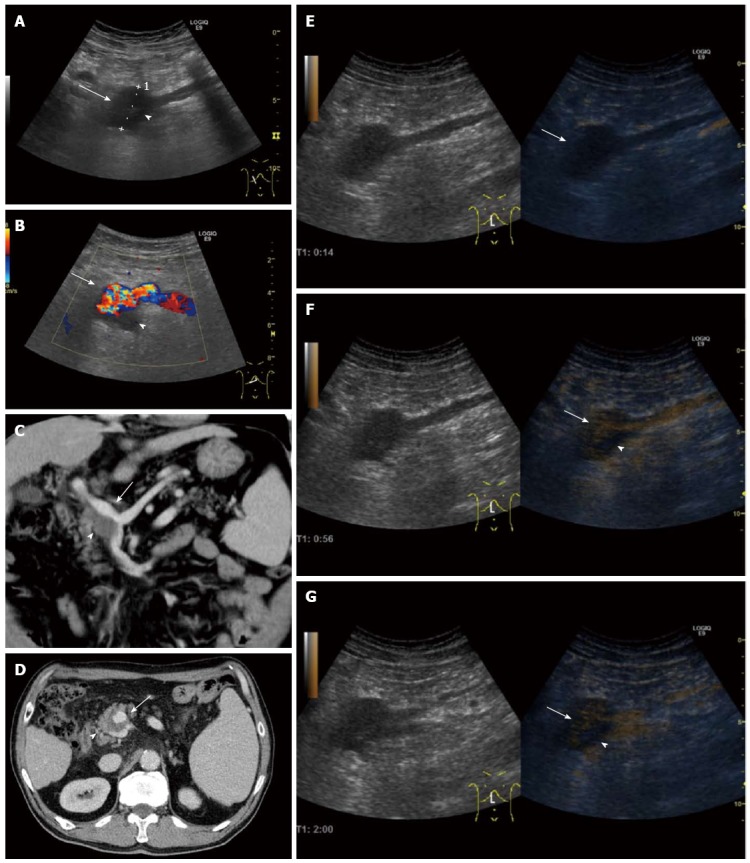
Methods: In this multi-center, retrospective, case series study, we evaluated CEUS features of seven cases of PVSAs that were found incidentally on conventional ultrasound in the period 2007-2013. Three Ultrasound Centers were involved (Chieti, Italy, Bad Mergentheim, Germany, and Cluj-Napoca, Romania). All patients underwent CEUS with Sonovue(®) (Bracco, Milan, Italy) at a standard dose of 2.4 mL, followed by 10 mL of 0.9% saline solution. The examinations were performed using multifrequency transducers and low mechanical index. We considered aneurysmal a focal dilatation of the portal venous system with a size that was significantly greater than the remaining segments of the same vein, and that was equal or larger than 21 mm for the extrahepatic segments of portal venous system, main portal vein and bifurcation, and 9 mm for the intrahepatic branches.
Results: After contrast agent injection, all PVSAs were not enhanced in the arterial phase (starting 8-22 s). All PVSAs were then rapidly enhanced in the early portal venous phase (starting three to five seconds after the arterial phase, 11-30 s), with persistence and slow washout of the contrast agent in the late phase (starting 120 s). In all patients, CEUS confirmed the presence of a "to-and-fro" flow by showing a swirling pattern within the dilatation in the early portal venous phase. CEUS also improved the delineation of the lumen, and was reliable in showing its patency degree and integrity of walls. In one patient, CEUS showed a partial enhancement of the lumen with a uniformly nonenhancing area in the portal venous and late phases, suggesting thrombosis.
Conclusion: In our case series, we found that CEUS could be useful in the assessment and follow-up of a PVSA. Further studies are needed to validate its diagnostic accuracy.
Keywords: Aneurysm; Computed tomography; Contrast-enhanced ultrasound; Magnetic resonance imaging; Portal vein; Venous system.
Figures


Similar articles
-
Diagnosis of benign and malignant portal vein thrombosis in cirrhotic patients with hepatocellular carcinoma: color Doppler US, contrast-enhanced US, and fine-needle biopsy.Abdom Imaging. 2006 Sep-Oct;31(5):537-44. doi: 10.1007/s00261-005-0150-x. Abdom Imaging. 2006. PMID: 16865315
-
Diagnosis of portal vein thrombosis discontinued with liver tumors in patients with liver cirrhosis and tumors by contrast-enhanced US: a pilot study.Eur J Radiol. 2010 Aug;75(2):185-8. doi: 10.1016/j.ejrad.2009.04.021. Epub 2009 May 22. Eur J Radiol. 2010. PMID: 19464131
-
A Milestone: Approval of CEUS for Diagnostic Liver Imaging in Adults and Children in the USA.Ultraschall Med. 2016 Jun;37(3):229-32. doi: 10.1055/s-0042-107411. Epub 2016 Jun 8. Ultraschall Med. 2016. PMID: 27276056 English.
-
Contrast-enhanced ultrasound in differentiating malignant from benign portal vein thrombosis in hepatocellular carcinoma.World J Gastroenterol. 2015 Aug 28;21(32):9457-60. doi: 10.3748/wjg.v21.i32.9457. World J Gastroenterol. 2015. PMID: 26327753 Free PMC article. Review.
-
Portal vein thrombosis in liver cirrhosis - the added value of contrast enhanced ultrasonography.Med Ultrason. 2016 Jun;18(2):218-33. doi: 10.11152/mu.2013.2066.182.pvt. Med Ultrason. 2016. PMID: 27239658 Review.
Cited by
-
Advantages and Limitations of Focal Liver Lesion Assessment with Ultrasound Contrast Agents: Comments on the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) Guidelines.Med Princ Pract. 2016;25(5):399-407. doi: 10.1159/000447670. Epub 2016 Jun 17. Med Princ Pract. 2016. PMID: 27318740 Free PMC article. Review.
-
Hepatic artery resistive index as surrogate marker for fibrosis progression in NAFLD patients: A clinical perspective.Int J Immunopathol Pharmacol. 2018 Jan-Dec;32:2058738418781373. doi: 10.1177/2058738418781373. Int J Immunopathol Pharmacol. 2018. PMID: 29873275 Free PMC article.
-
Vascular Diseases of the Spleen: A Review.J Clin Transl Hepatol. 2017 Jun 28;5(2):152-164. doi: 10.14218/JCTH.2016.00062. Epub 2017 Mar 24. J Clin Transl Hepatol. 2017. PMID: 28660153 Free PMC article. Review.
-
Role of contrast-enhanced ultrasound (CEUS) in the diagnosis of endometrial pathology.Clujul Med. 2015;88(4):433-7. doi: 10.15386/cjmed-499. Epub 2015 Nov 15. Clujul Med. 2015. PMID: 26733740 Free PMC article. Review.
References
-
- Koc Z, Oguzkurt L, Ulusan S. Portal venous system aneurysms: imaging, clinical findings, and a possible new etiologic factor. AJR Am J Roentgenol. 2007;189:1023–1030. - PubMed
-
- Ohnishi K, Nakayama T, Saito M, Nomura F, Koen H, Tamaru J, Iwasaki I, Okuda K. Aneurysm of the intrahepatic branch of the portal vein. Report of two cases. Gastroenterology. 1984;86:169–173. - PubMed
-
- Barzilai R, Kleckner MS. Hemocholecyst following ruptured aneurysm of portal vein; report of a case. AMA Arch Surg. 1956;72:725–727. - PubMed
-
- Piscaglia F, Nolsøe C, Dietrich CF, Cosgrove DO, Gilja OH, Bachmann Nielsen M, Albrecht T, Barozzi L, Bertolotto M, Catalano O, et al. The EFSUMB Guidelines and Recommendations on the Clinical Practice of Contrast Enhanced Ultrasound (CEUS): update 2011 on non-hepatic applications. Ultraschall Med. 2012;33:33–59. - PubMed
-
- Dietrich CF, Averkiou MA, Correas JM, Lassau N, Leen E, Piscaglia F. An EFSUMB introduction into Dynamic Contrast-Enhanced Ultrasound (DCE-US) for quantification of tumour perfusion. Ultraschall Med. 2012;33:344–351. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
