

Association between 7 years of intensive treatment of type 1 diabetes and long-term mortality
- PMID: 25562265
- PMCID: PMC4306335
- DOI: 10.1001/jama.2014.16107
Association between 7 years of intensive treatment of type 1 diabetes and long-term mortality
Abstract
Importance: Whether mortality in type 1 diabetes mellitus is affected following intensive glycemic therapy has not been established.
Objective: To determine whether mortality differed between the original intensive and conventional treatment groups in the long-term follow-up of the Diabetes Control and Complications Trial (DCCT) cohort.
Design, setting, and participants: After the DCCT (1983-1993) ended, participants were followed up in a multisite (27 US and Canadian academic clinical centers) observational study (Epidemiology of Diabetes Control and Complications [EDIC]) until December 31, 2012. Participants were 1441 healthy volunteers with diabetes mellitus who, at baseline, were 13 to 39 years of age with 1 to 15 years of diabetes duration and no or early microvascular complications, and without hypertension, preexisting cardiovascular disease, or other potentially life-threatening disease.
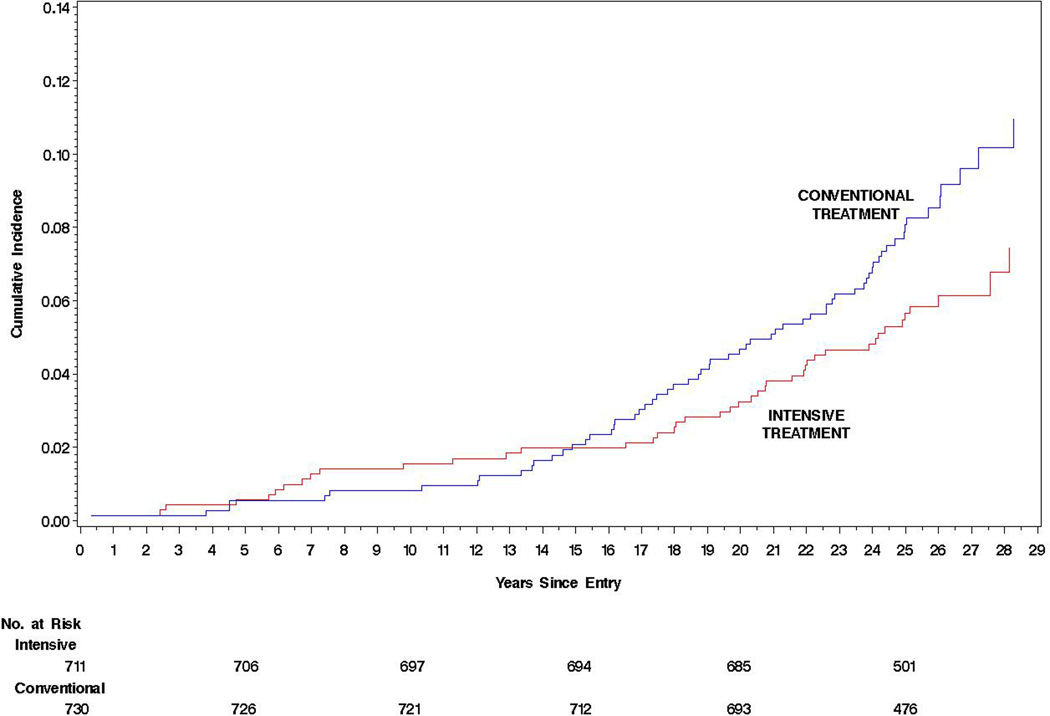
Interventions and exposures: During the clinical trial, participants were randomly assigned to receive intensive therapy (n = 711) aimed at achieving glycemia as close to the nondiabetic range as safely possible, or conventional therapy (n = 730) with the goal of avoiding symptomatic hypoglycemia and hyperglycemia. At the end of the DCCT, after a mean of 6.5 years, intensive therapy was taught and recommended to all participants and diabetes care was returned to personal physicians.
Main outcomes and measures: Total and cause-specific mortality was assessed through annual contact with family and friends and through records over 27 years' mean follow-up.
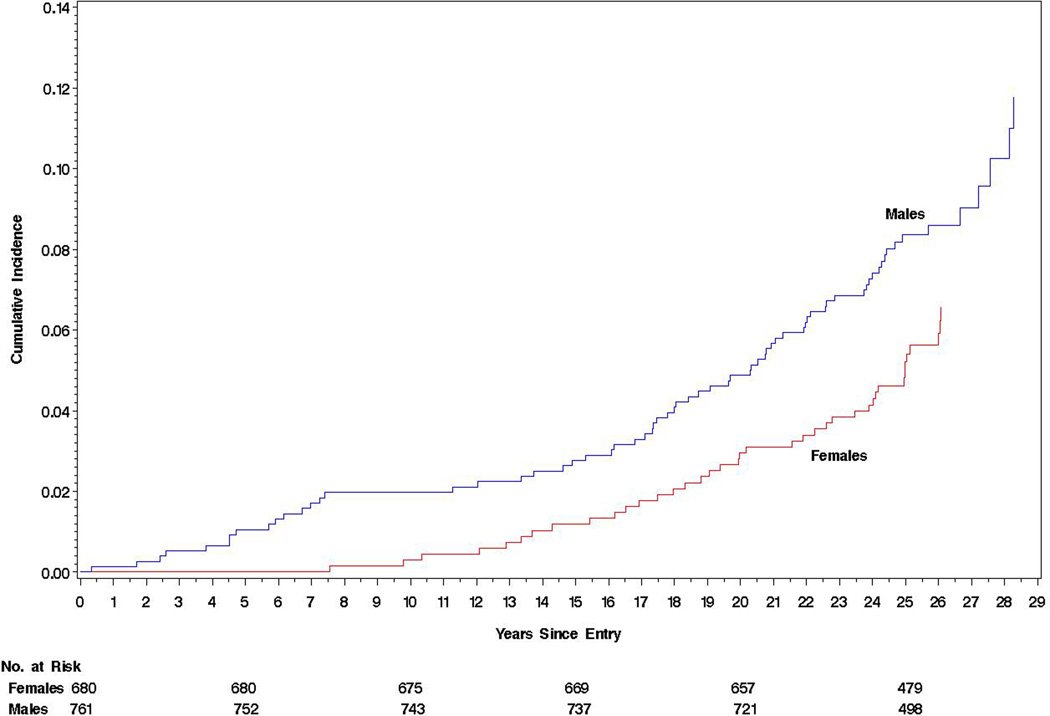
Results: Vital status was ascertained for 1429 (99.2%) participants. There were 107 deaths, 64 in the conventional and 43 in the intensive group. The absolute risk difference was -109 per 100,000 patient-years (95% CI, -218 to -1), with lower all-cause mortality risk in the intensive therapy group (hazard ratio [HR] = 0.67 [95% CI, 0.46-0.99]; P = .045). Primary causes of death were cardiovascular disease (24 deaths; 22.4%), cancer (21 deaths; 19.6%), acute diabetes complications (19 deaths; 17.8%), and accidents or suicide (18 deaths; 16.8%). Higher levels of glycated hemoglobin (HbA1c) were associated with all-cause mortality (HR = 1.56 [95% CI, 1.35-1.81 per 10% relative increase in HbA1c]; P < .001), as well as the development of albuminuria (HR = 2.20 [95% CI, 1.46-3.31]; P < .001).
Conclusions and relevance: After a mean of 27 years' follow-up of patients with type 1 diabetes, 6.5 years of initial intensive diabetes therapy was associated with a modestly lower all-cause mortality rate when compared with conventional therapy.
Trial registration: clinicaltrials.gov Identifiers: NCT00360815 and NCT00360893.
Conflict of interest statement
Figures
Comment in
-
Mortality in type 1 diabetes in the current era: two steps forward, one step backward.JAMA. 2015 Jan 6;313(1):35-6. doi: 10.1001/jama.2014.16327. JAMA. 2015. PMID: 25562263 No abstract available.
-
Intensive treatment for type 1 diabetes is associated with lower risk of death.BMJ. 2015 Jan 6;350:h32. doi: 10.1136/bmj.h32. BMJ. 2015. PMID: 25566784 No abstract available.
-
ACP Journal Club. In type 1 diabetes, intensive insulin therapy for 6.5 y reduced mortality at 27 y compared with usual care.Ann Intern Med. 2015 May 19;162(10):JC12. doi: 10.7326/ACPJC-2015-162-10-012. Ann Intern Med. 2015. PMID: 25984873 No abstract available.
References
-
- Borch-Johnsen K, Kreiner S, Deckert T. Mortality of type 1 (insulin-dependent) diabetes mellitus in Denmark: a study of relative mortality in 2930 Danish type 1 diabetic patients diagnosed from 1933 to 1972. Diabetologia. 1986;29(11):767–772. - PubMed
-
- Skrivarhaug T, Bangstad HJ, Stene LC, Sandvik L, Hanssen KF, Joner G. Long-term mortality in a nationwide cohort of childhood-onset type 1 diabetic patients in Norway. Diabetologia. 2006;49(2):298–305. - PubMed
-
- Soedamah-Muthu SS, Fuller JH, Mulnier HE, Raleigh VS, Lawrenson RA, Colhoun HM. All-cause mortality rates in patients with type 1 diabetes mellitus compared with a non-diabetic population from the UK general practice research database, 1992–1999. Diabetologia. 2006;49:660–666. - PubMed
-
- Shankar A, Klein R, Klein BEK, Moss SE. Association between glycosylated hemoglobin level and cardiovascular and all-cause mortality in type 1 diabetes. Am J Epidemiol. 2007;166(4):393–402. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
