

Economic evaluation of a pharmaceutical care program for elderly diabetic and hypertensive patients in primary health care: a 36-month randomized controlled clinical trial
- PMID: 25562774
- PMCID: PMC10398185
- DOI: 10.18553/jmcp.2015.21.1.66
Economic evaluation of a pharmaceutical care program for elderly diabetic and hypertensive patients in primary health care: a 36-month randomized controlled clinical trial
Abstract
Background: Most diabetic and hypertensive patients, principally the elderly, do not achieve adequate disease control and consume 5%-15% of annual health care budgets. Previous studies verified that pharmaceutical care is useful for achieving adequate disease control in diabetes and hypertension.
Objective: To evaluate the economic cost and the incremental cost-effectiveness ratio (ICER) per quality-adjusted life-year (QALY) of pharmaceutical care in the management of diabetes and hypertension in elderly patients in a primary public health care system in a developing country.
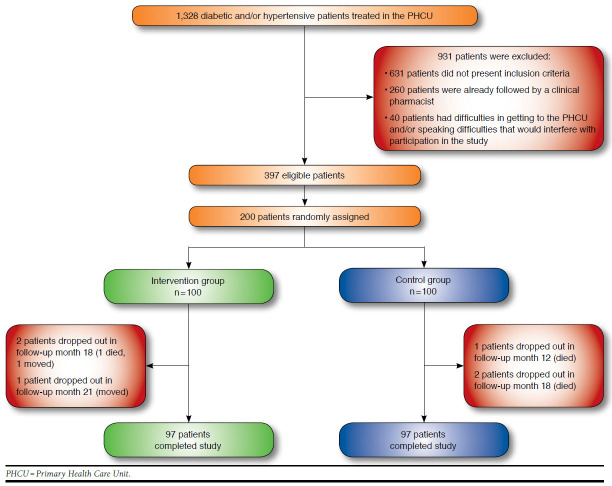
Methods: A 36-month randomized controlled clinical trial was performed with 200 patients who were divided into a control group (n = 100) and an intervention group (n = 100). The control group received the usual care offered by the Primary Health Care Unit (medical and nurse consultations). The intervention group received the usual care plus a pharmaceutical care intervention. The intervention and control groups were compared with regard to the direct costs of health services (i.e., general practitioner, specialist, nurse, and pharmacist appointments; emergency room visits; and drug therapy costs) and the ICER per QALY. These evaluations used the health system perspective.
Results: No statistically significant difference was found between the intervention and control groups in total direct health care costs ($281.97 ± $49.73 per patient vs. $212.28 ± $43.49 per patient, respectively; P = 0.089); pharmaceutical care added incremental costs of $69.60 (± $7.90) per patient. The ICER per QALY was $53.50 (95% CI = $51.60-$54.00; monetary amounts are given in U.S. dollars). Every clinical parameter evaluated improved for the pharmaceutical care group, whereas these clinical parameters remained unchanged in the usual care group. The difference in differences (DID) tests indicated that for each clinical parameter, the patients in the intervention group improved more from pre to post than the control group (P < 0.001).
Conclusions: While pharmaceutical care did not significantly increase total direct health care costs, significantly improved health outcomes were seen. The mean ICER per QALY gained suggests a favorable cost-effectiveness.
Conflict of interest statement
The authors report no conflicts of interest regarding this study. No separate funding was obtained for this study.
Study concept and design were contributed by Obreli-Neto and Cuman. Obreli-Neto had primary responsibility for data collection; data interpretation was primarily the work of Obreli-Neto, Leira, Guidoni, Baldoni, Marusic, Renovato, Pilger, and Cuman. The manuscript was written primarily by Obreli-Neto, with assistance from Marusic, Guidoni, Leira, Baldoni, and Cuman, and was revised by Renovato, Baldoni, Guidoni, Leira, Pilger, and Marusic.
References
-
- International Diabetes Federation. IDF Diabetes Atlas. 6th ed. Brussels, Belgium: International Diabetes Federation; 2013. Available at: http://www.idf.org/sites/default/files/EN_6E_Atlas_Full_0.pdf. Accessed December 8, 2014.
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365(9455):217-23. - PubMed
-
- Stark Casagrande S, Fradkin JE, Saydah SH, Rust KF, Cowie CC. The prevalence of meeting A1c, blood pressure, and LDL goals among people with diabetes, 1988-2010. Diabetes Care. 2013;36(8):2271-79. Available at: http://care.diabetesjournals.org/content/36/8/2271.full.pdf+html. Accessed December 8, 2014. - PMC - PubMed
-
- Pereira M, Lunet N, Azevedo A, Barros H. Differences in prevalence, awareness, treatment and control of hypertension between developing and developed countries. J Hypertens. 2009;27(5):963-75. - PubMed
-
- Moreira GC, Cipullo JP, Martin JF, et al. . Evaluation of the awareness, control and cost-effectiveness of hypertension treatment in a Brazilian city: populational study. J Hypertens. 2009;27(9):1900-07. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
