

Population-based surveillance of HIV drug resistance emerging on treatment and associated factors at sentinel antiretroviral therapy sites in Namibia
- PMID: 25564107
- PMCID: PMC4334707
- DOI: 10.1097/QAI.0000000000000509
Population-based surveillance of HIV drug resistance emerging on treatment and associated factors at sentinel antiretroviral therapy sites in Namibia
Abstract
Objective: The World Health Organization (WHO) prospective surveys of acquired HIV drug resistance (HIVDR) evaluate HIVDR emerging after the first year of antiretroviral therapy (ART) and associated factors.
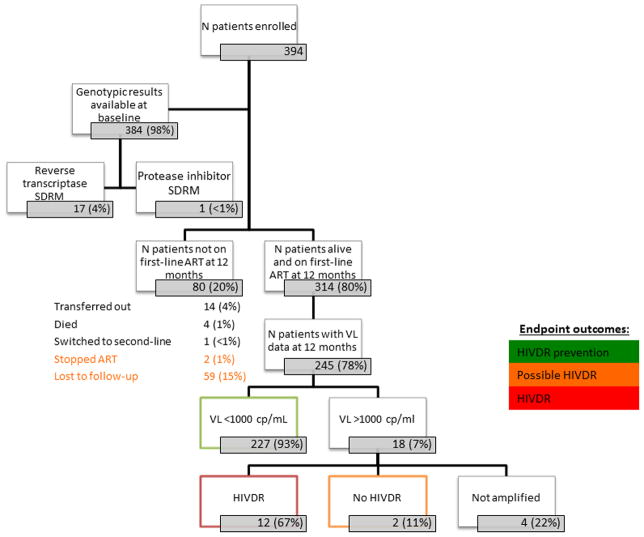
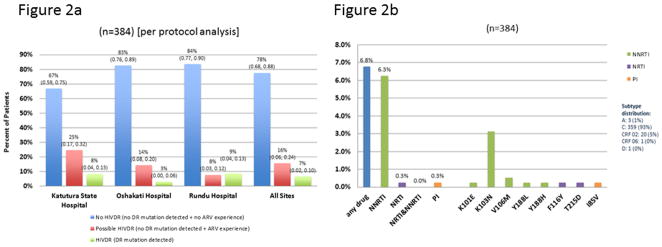
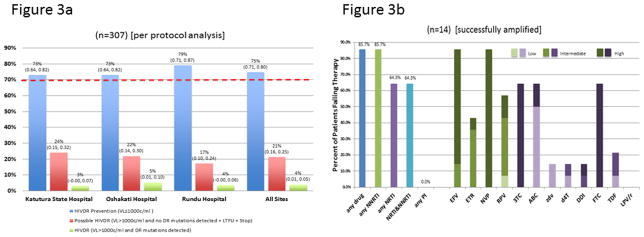
Methods: Consecutive ART starters in 2009 were enrolled at 3 sentinel sites in Namibia. Genotyping was performed at start and after 12 months in patients with HIV viral load (VL) >1000 copies per mL. HIVDR outcomes were: HIVDR prevention (VL ≤1000 copies/mL), possible HIVDR (VL >1000 copies/mL without detectable HIVDR or loss to follow-up or ART stop), and HIVDR (VL >1000 copies/mL with detectable HIVDR). Adherence was assessed using medication possession ratio (MPR).
Results: Of 394 starters, at 12 months, 80% were on first-line ART, 1% died, 4% transferred out, 1% stopped ART, <1% switched to second-line, and 15% were lost to follow-up. Among patients on first-line, 77% had VL testing, and 94% achieved VL ≤1000 copies per mL. At baseline, 7% had HIVDR. After 12 months, among patients with VL testing, 5% had HIVDR. A majority of patients failing therapy had high-level resistance to nonnucleoside reverse transcriptase inhibitors but none to protease inhibitors. All sites achieved the WHO target of ≥70% HIVDR prevention. Factors associated with not achieving HIVDR prevention were: baseline resistance to nonnucleoside reverse transcriptase inhibitors [odds ratio (OR) 3.0, P = 0.023], WHO stage 3 or 4 at baseline (OR 2.0, P = 0.012), and MPR <75% (OR 4.9, P = 0.021).
Conclusions: Earlier ART initiation and removal of barriers to on-time drug pickups may help to prevent HIVDR. These data inform decisions at national and global levels on the effectiveness of first- and second-line regimens.
Conflict of interest statement
Figures
References
-
- Gilks CF, Crowley S, Ekpini R, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–10. - PubMed
-
- World Health Organization. [Accessed 4 August 2014];WHO global strategy for the surveillance and monitoring of HIV drug resistance. 2012 http://www.who.int/hiv/pub/drugresistance/drug_resistance_strategy/en/in....
-
- Central Intelligence Agency. Namibia. [Accessed 4 August 2014];The World Factbook. 2014 https://www.cia.gov/library/publications/the-world-factbook/geos/wa.html.
-
- Republic of Namibia Ministry of Health and Social Services. Report on the 2012 National HIV Sentinel Survey
-
- Republic of Namibia Ministry of Health and Social Services Directorate of Special Programs. [Accessed 18 October 2011];National Guidelines for Antiretroviral Therapy. (3). 2010 http://www.who.int/hiv/pub/guidelines/namibia_art.pdf.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
