

Evaluating controlled human malaria infection in Kenyan adults with varying degrees of prior exposure to Plasmodium falciparum using sporozoites administered by intramuscular injection
- PMID: 25566206
- PMCID: PMC4264479
- DOI: 10.3389/fmicb.2014.00686
Evaluating controlled human malaria infection in Kenyan adults with varying degrees of prior exposure to Plasmodium falciparum using sporozoites administered by intramuscular injection
Abstract
Background: Controlled human malaria infection (CHMI) studies are a vital tool to accelerate vaccine and drug development. As CHMI trials are performed in a controlled environment, they allow unprecedented, detailed evaluation of parasite growth dynamics (PGD) and immunological responses. However, CHMI studies have not been routinely performed in malaria-endemic countries or used to investigate mechanisms of naturally-acquired immunity (NAI) to Plasmodium falciparum.
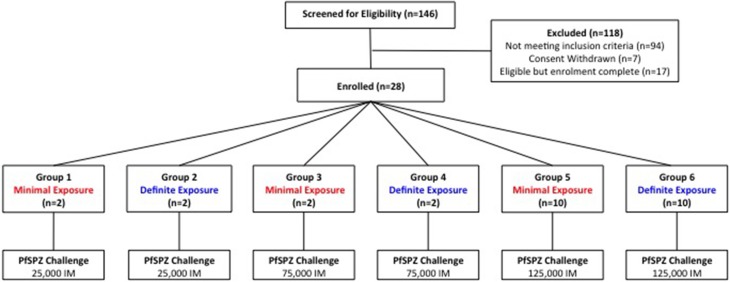
Methods: We conducted an open-label, randomized CHMI pilot-study using aseptic, cryopreserved P. falciparum sporozoites (PfSPZ Challenge) to evaluate safety, infectivity and PGD in Kenyan adults with low to moderate prior exposure to P. falciparum (Pan African Clinical Trial Registry: PACTR20121100033272).
Results: All participants developed blood-stage infection confirmed by quantitative polymerase chain reaction (qPCR). However one volunteer (110) remained asymptomatic and blood-film negative until day 21 post-injection of PfSPZ Challenge. This volunteer had a reduced parasite multiplication rate (PMR) (1.3) in comparison to the other 27 volunteers (median 11.1). A significant correlation was seen between PMR and screening anti-schizont Enzyme Linked Immunosorbent Assays (ELISA) OD (p = 0.044, R = -0.384) but not when volunteer 110 was excluded from the analysis (p = 0.112, R = -0.313).
Conclusions: PfSPZ Challenge is safe and infectious in malaria-endemic populations and could be used to assess the efficacy of malaria vaccines and drugs in African populations. Whilst our findings are limited by sample size, our pilot study has demonstrated for the first time that NAI may impact on PMR post-CHMI in a detectable fashion, an important finding that should be evaluated in further CHMI studies.
Keywords: CHMI; challenge; falciparum; immunity; malaria.
Figures





References
-
- Bray R. S., Gunders A. E., Burgess R. W., Freeman J. B., Etzel E., Guttuso C., et al. . (1962). The inoculation of semi-immune Africans with sporozoites of Laverania falcipara (Plasmodium falciparum) in Liberia. Riv. Malariol. 41, 199–210. - PubMed
-
- Bruce-Chwatt L. J. (1963a). A longitudinal longitudinal survey of natural malaria infection in a group of West African adults. I. West Afr. Med. J. 12, 141–173. - PubMed
-
- Bruce-Chwatt L. J. (1963b). A longitudinal survey of natural malaria infection in a group of West African adults. West Afr. Med. J. 12, 199–217. - PubMed
-
- Chulay J. D., Schneider I., Cosgriff T. M., Hoffman S. L., Ballou W. R., Quakyi I. A., et al. . (1986). Malaria transmitted to humans by mosquitoes infected from cultured Plasmodium falciparum. Am. J. Trop. Med. Hyg. 35, 66–68. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous