

Alteration of immunoproteome profile of Echinococcus granulosus hydatid fluid with progression of cystic echinococcosis
- PMID: 25566682
- PMCID: PMC4311513
- DOI: 10.1186/s13071-014-0610-7
Alteration of immunoproteome profile of Echinococcus granulosus hydatid fluid with progression of cystic echinococcosis
Abstract
Background: Cystic echinococcosis (CE), caused by Echinococcus granulosus metacestode, invokes a serious public health concern. Early diagnosis has great impacts on reduction of disability-adjusted life years. Several antigen B-related molecules (EgAgB; EgAgB1-5) are known to be immunopotent, but detection of EgAgB is variable in many patients and may not allow reliable interpretation of its immunological relevance. More importantly, the immunoproteome profile of hydatid fluid (HF) has not been addressed.
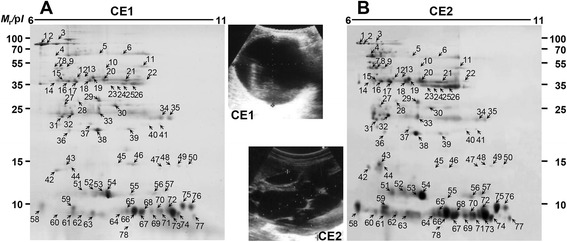
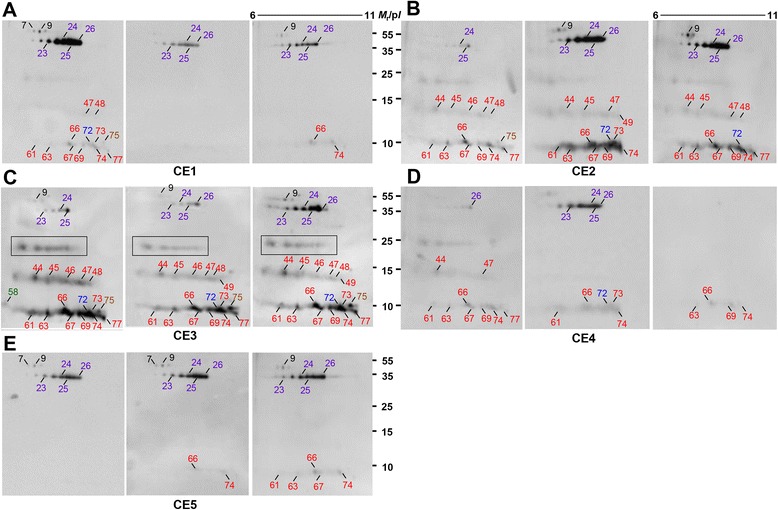
Methods: We conducted a proteome analysis of the HF of a single fertile cyst of CE1 and CE2 stages through two-dimensional electrophoresis (2-DE). Each protein spot was analyzed by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS). We subsequently determined the immunoproteome profile employing patient sera of entire disease spectrum from CE1 to CE5 stages.
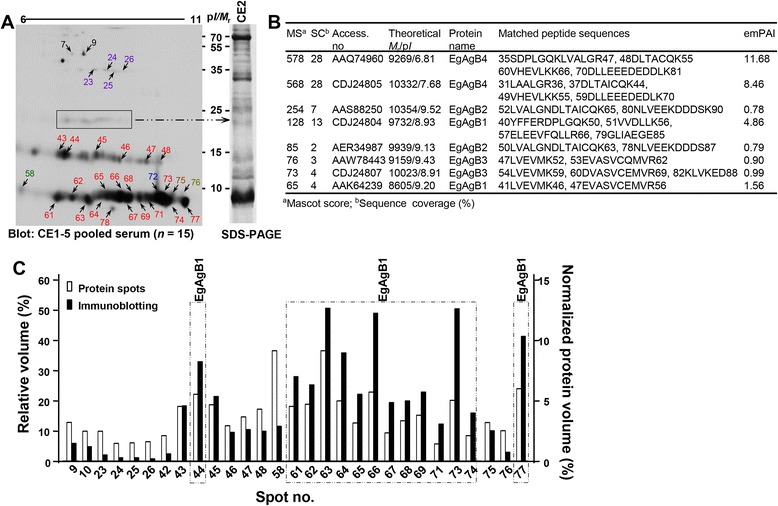
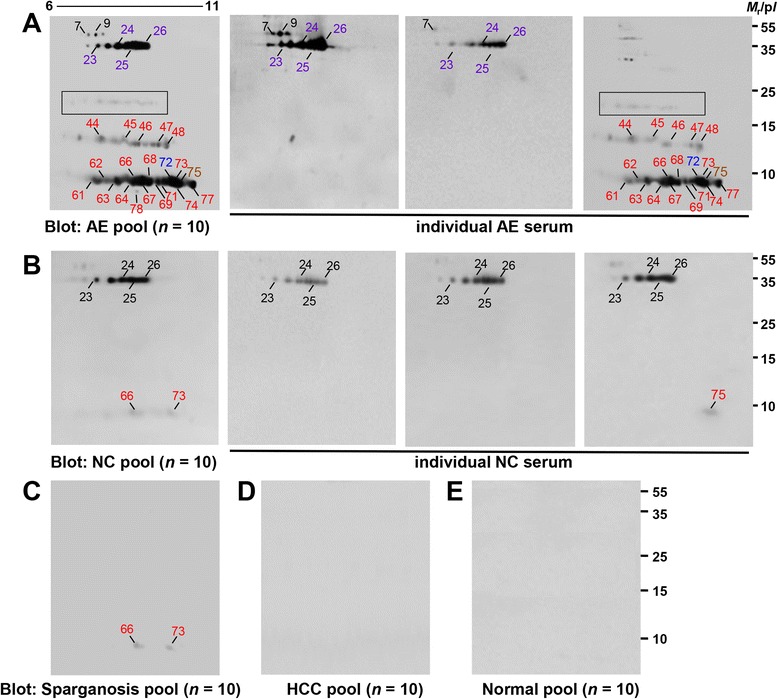
Results: We identified 40 parasite proteins, of which EgAgB (28 spots) and antigen 5 (EgAg5; 5 molecules) were abundant. EgAgB proteoforms constituted the majority, mostly EgAgB1 (24 spots), followed by EgAgB2 and EgAgB4 (2 spots each). EgAgB3 was detected only by liquid chromatography-MS/MS. EgAgB5 was not recognized. We also detected 38 host proteins, which were largely composed of serum components, antioxidant/xenobiotic enzymes, and enzymes involved in carbohydrate metabolism. CE1 and CE2 HF exhibited comparable spotting patterns, but CE2 HF harbored greater amounts of EgAgB and EgAg5 complexes. CE sera demonstrated complicated immune recognition patterns according to the disease progression; CE2 and CE3 stages exhibited strong antibody responses against diverse EgAgB and EgAg5 proteoforms, while CE1, CE4, and CE5 stages mainly reacted to EgAg5 and cathepsin B. Patient sera of alveolar echinococcosis (AE) cross-reacted with diverse EgAgB isoforms (36%). EgAg5 and cathepsin B also demonstrated cross-reactions with sera from neurocysticercosis and sparganosis.
Conclusions: Our results demonstrated that detection of a single defined molecule may not properly diagnose CE, since specific immunodominant epitopes changed as the disease progresses. Immunoproteome analysis combined with imaging studies may be practical in the differential diagnosis of CE from AE and other cystic lesions, as well as for staging CE, which are pertinent to establish appropriate patient management.
Figures
References
-
- Zhang W, Zhang Z, Wu W, Shi B, Li J, Zhou X, Wen H, McManus DP: Epidemiology and control of echinococcosis in central Asia, with particular reference to the People’s Republic of China.Acta Trop 2014. http://dx.doi.org/10.1016/j.actatropica.2014.03.014. - PubMed
-
- Yang YR, Clements AC, Gray DJ, Atkinson JA, Williams GM, Barnes TS, McManus DP. Impact of anthropogenic and natural environmental changes on Echinococcus transmission in Ningxia Hui Autonomous Region, the People’s Republic of China. Parasit Vectors. 2012;5:146. doi: 10.1186/1756-3305-5-146. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
