

Antimicrobial heteroresistance: an emerging field in need of clarity
- PMID: 25567227
- PMCID: PMC4284305
- DOI: 10.1128/CMR.00058-14
Antimicrobial heteroresistance: an emerging field in need of clarity
Abstract
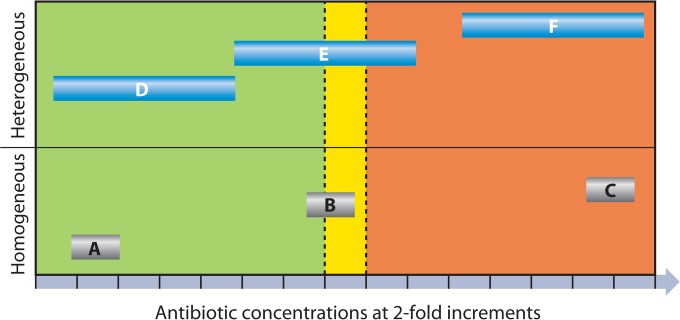
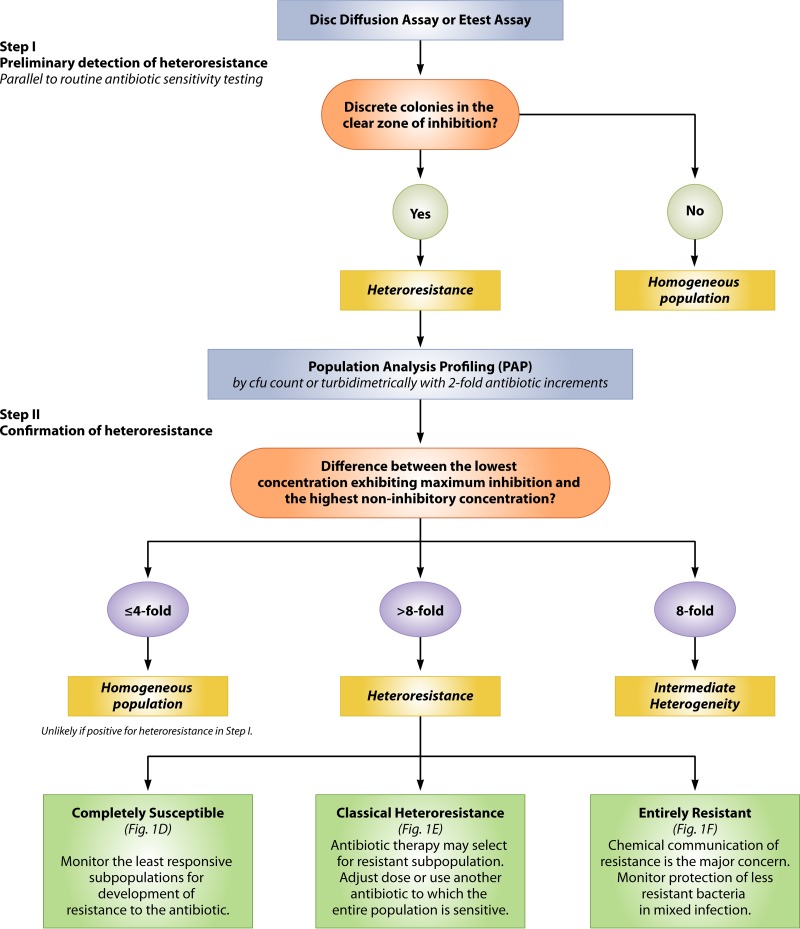
"Heteroresistance" describes a phenomenon where subpopulations of seemingly isogenic bacteria exhibit a range of susceptibilities to a particular antibiotic. Unfortunately, a lack of standard methods to determine heteroresistance has led to inappropriate use of this term. Heteroresistance has been recognized since at least 1947 and occurs in Gram-positive and Gram-negative bacteria. Its clinical relevance may be considerable, since more resistant subpopulations may be selected during antimicrobial therapy. However, the use of nonstandard methods to define heteroresistance, which are costly and involve considerable labor and resources, precludes evaluating the clinical magnitude and severity of this phenomenon. We review the available literature on antibiotic heteroresistance and propose recommendations for definitions and determination criteria for heteroresistant bacteria. This will help in assessing the global clinical impact of heteroresistance and developing uniform guidelines for improved therapeutic outcomes.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures


References
-
- CDC. 2013. Antibiotic resistance threats in the United States, 2013. US Department of Health and Human Services, Centers for Disease Control and Prevention, Atlanta, GA.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
