

Heparin binding-epidermal growth factor-like growth factor for the regeneration of chronic tympanic membrane perforations in mice
- PMID: 25567607
- PMCID: PMC4426296
- DOI: 10.1089/ten.TEA.2014.0474
Heparin binding-epidermal growth factor-like growth factor for the regeneration of chronic tympanic membrane perforations in mice
Abstract
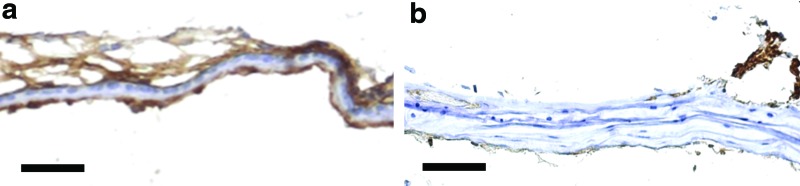
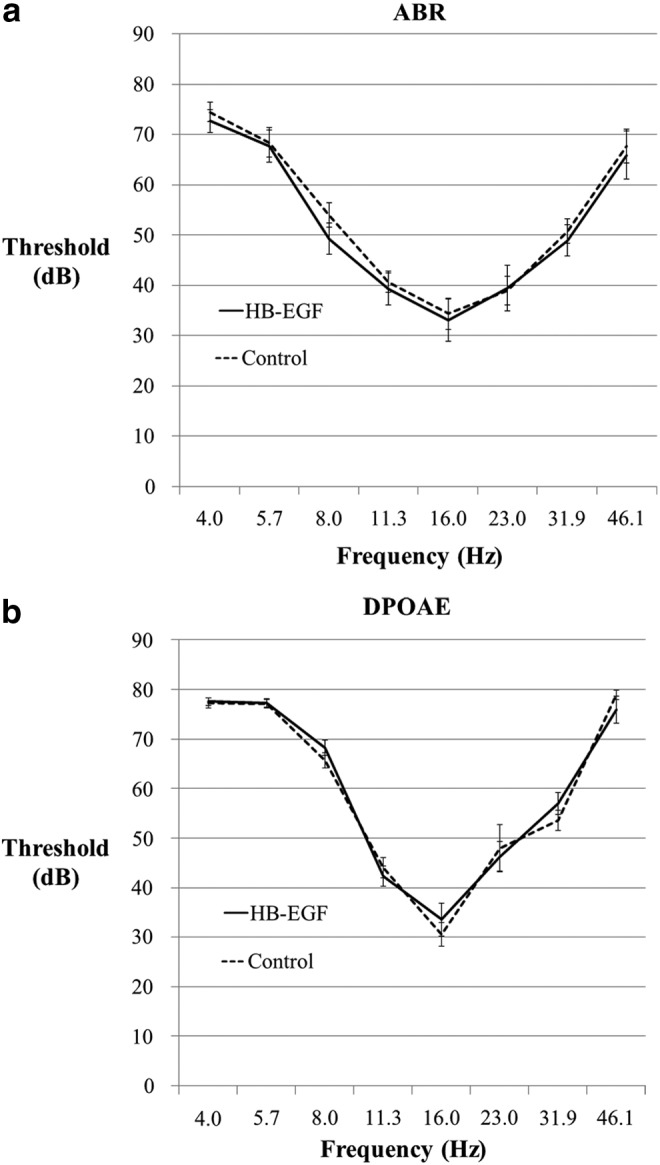
We aim to explore the role of epidermal growth factor (EGF) ligand shedding in tympanic membrane wound healing and to investigate the translation of its modulation in tissue engineering of chronic tympanic membrane perforations. Chronic suppurative otitis media (CSOM) is an infected chronic tympanic membrane perforation. Up to 200 million suffer from its associated hearing loss and it is the most common cause of pediatric hearing loss in developing countries. There is a need for nonsurgical treatment due to a worldwide lack of resources. In this study, we show that EGF ligand shedding is essential for tympanic membrane healing as it's inhibition, with KB-R7785, leads to chronic perforation in 87.9% (n=58) compared with 0% (n=20) of controls. We then show that heparin binding-EGF-like growth factor (5 μg/mL), which acts to shed EGF ligands, can regenerate chronic perforations in mouse models with 92% (22 of 24) compared with 38% (10 of 26), also with eustachian tube occlusion with 94% (18 of 19) compared with 9% (2 of 23) and with CSOM 100% (16 of 16) compared with 41% (7 of 17). We also show the nonototoxicity of this treatment and its hydrogel delivery vehicle. This provides preliminary data for a clinical trial where it could be delivered by nonspecialist trained healthcare workers and fulfill the clinical need for a nonsurgical treatment for chronic tympanic membrane perforation and CSOM.
Figures
Comment in
-
In Response to: Heparin Binding-Epidermal Growth Factor-Like Growth Factor for the Regeneration of Chronic Tympanic Membrane Perforations in Mice.Tissue Eng Part A. 2016 Mar;22(5-6):568-9. doi: 10.1089/ten.TEA.2016.0040. Epub 2016 Mar 9. Tissue Eng Part A. 2016. PMID: 26879548 No abstract available.
-
In Response to the Letter to the Editor Regarding: Heparin Binding-Epidermal Growth Factor-Like Growth Factor for the Regeneration of Chronic Tympanic Membrane Perforations in Mice.Tissue Eng Part A. 2016 Mar;22(5-6):570-1. doi: 10.1089/ten.TEA.2016.0059. Tissue Eng Part A. 2016. PMID: 26908042 No abstract available.
Similar articles
-
Heparin Binding Epidermal Growth Factor-Like Growth Factor Heals Chronic Tympanic Membrane Perforations With Advantage Over Fibroblast Growth Factor 2 and Epidermal Growth Factor in an Animal Model.Otol Neurotol. 2015 Aug;36(7):1279-83. doi: 10.1097/MAO.0000000000000795. Otol Neurotol. 2015. PMID: 26075672 Free PMC article.
-
Functional Outcomes of Heparin-Binding Epidermal Growth Factor-Like Growth Factor for Regeneration of Chronic Tympanic Membrane Perforations in Mice.Tissue Eng Part A. 2017 May;23(9-10):436-444. doi: 10.1089/ten.TEA.2016.0395. Epub 2017 Feb 24. Tissue Eng Part A. 2017. PMID: 28142401 Free PMC article.
-
In Response to: Heparin Binding-Epidermal Growth Factor-Like Growth Factor for the Regeneration of Chronic Tympanic Membrane Perforations in Mice.Tissue Eng Part A. 2016 Mar;22(5-6):568-9. doi: 10.1089/ten.TEA.2016.0040. Epub 2016 Mar 9. Tissue Eng Part A. 2016. PMID: 26879548 No abstract available.
-
A moist edge environment aids the regeneration of traumatic tympanic membrane perforations.J Laryngol Otol. 2017 Jul;131(7):564-571. doi: 10.1017/S0022215117001001. Epub 2017 May 15. J Laryngol Otol. 2017. PMID: 28502255 Review.
-
Chronic tympanic membrane perforation: a better animal model is needed.Wound Repair Regen. 2007 Jul-Aug;15(4):450-8. doi: 10.1111/j.1524-475X.2007.00251.x. Wound Repair Regen. 2007. PMID: 17650087 Review.
Cited by
-
Manufacturing Radially Aligned PCL Nanofibers Reinforced With Sulfated Levan and Evaluation of its Biological Activity for Healing Tympanic Membrane Perforations.Macromol Biosci. 2025 Jan;25(1):e2400291. doi: 10.1002/mabi.202400291. Epub 2024 Oct 26. Macromol Biosci. 2025. PMID: 39461894 Free PMC article.
-
Heparin Binding Epidermal Growth Factor-Like Growth Factor Heals Chronic Tympanic Membrane Perforations With Advantage Over Fibroblast Growth Factor 2 and Epidermal Growth Factor in an Animal Model.Otol Neurotol. 2015 Aug;36(7):1279-83. doi: 10.1097/MAO.0000000000000795. Otol Neurotol. 2015. PMID: 26075672 Free PMC article.
-
Heparin-Binding Epidermal Growth Factor-Like Growth Factor as a Critical Mediator of Tissue Repair and Regeneration.Am J Pathol. 2018 Nov;188(11):2446-2456. doi: 10.1016/j.ajpath.2018.07.016. Epub 2018 Aug 22. Am J Pathol. 2018. PMID: 30142332 Free PMC article. Review.
-
Epithelial separation theory for post-tonsillectomy secondary hemorrhage: evidence in a mouse model and potential heparin-binding epidermal growth factor-like growth factor therapy.Eur Arch Otorhinolaryngol. 2018 Feb;275(2):569-578. doi: 10.1007/s00405-017-4810-6. Epub 2017 Nov 29. Eur Arch Otorhinolaryngol. 2018. PMID: 29188436
-
Panel 1: Biotechnology, biomedical engineering and new models of otitis media.Int J Pediatr Otorhinolaryngol. 2020 Mar;130 Suppl 1(Suppl 1):109833. doi: 10.1016/j.ijporl.2019.109833. Epub 2019 Dec 27. Int J Pediatr Otorhinolaryngol. 2020. PMID: 31901291 Free PMC article. Review.
References
-
- Acuin J.Chronic Suppurative Otitis Media: Burden of Illness and Management Options. Switzerland: World Health Organisation, 2004
-
- Karela M., Berry S., Watkins A., and Phillipps JJ.Myringoplasty: surgical outcomes and hearing improvement: is it worth performing to improve hearing? Eur Arch Otorhinolaryngol 265,1039, 2008 - PubMed
-
- Aggarwal R., Saeed S.R., and Green K.J.Myringoplasty. J Laryngol Otol 120,429, 2006 - PubMed
-
- Jackler R.K.A regenerative method of tympanic membrane repair could be the greatest advance in otology since the cochlear implant. Otol Neurotol 33,289, 2012 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
