

Tumors: wounds that do not heal-redux
- PMID: 25568067
- PMCID: PMC4288010
- DOI: 10.1158/2326-6066.CIR-14-0209
Tumors: wounds that do not heal-redux
Abstract
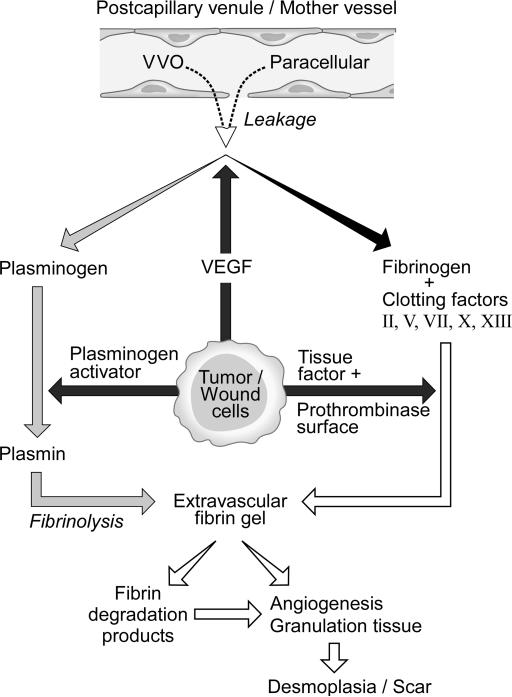
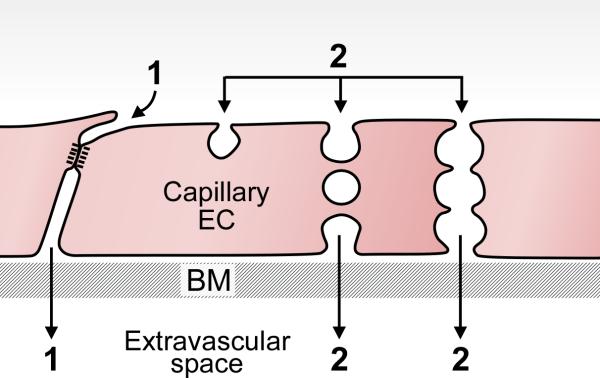
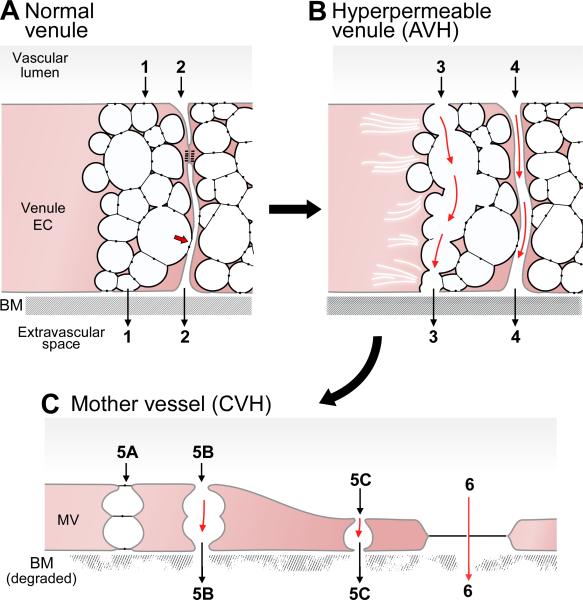
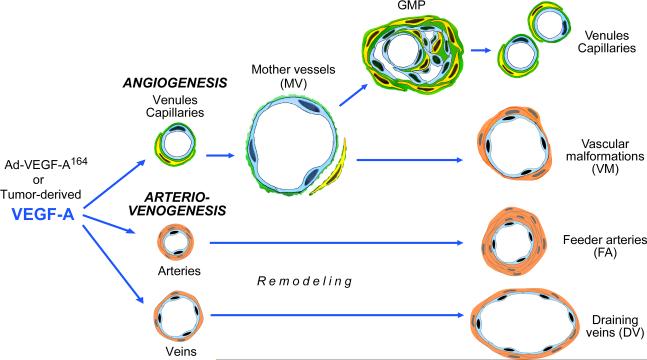
Similarities between tumors and the inflammatory response associated with wound healing have been recognized for more than 150 years and continue to intrigue. Some years ago, based on our then recent discovery of vascular permeability factor (VPF)/VEGF, I suggested that tumors behaved as wounds that do not heal. More particularly, I proposed that tumors co-opted the wound-healing response to induce the stroma they required for maintenance and growth. Work over the past few decades has supported this hypothesis and has put it on a firmer molecular basis. In outline, VPF/VEGF initiates a sequence of events in both tumors and wounds that includes the following: increased vascular permeability; extravasation of plasma, fibrinogen and other plasma proteins; activation of the clotting system outside the vascular system; deposition of an extravascular fibrin gel that serves as a provisional stroma and a favorable matrix for cell migration; induction of angiogenesis and arterio-venogenesis; subsequent degradation of fibrin and its replacement by "granulation tissue" (highly vascular connective tissue); and, finally, vascular resorption and collagen synthesis, resulting in the formation of dense fibrous connective tissue (called "scar tissue" in wounds and "desmoplasia" in cancer). A similar sequence of events also takes place in a variety of important inflammatory diseases that involve cellular immunity.
©2015 American Association for Cancer Research.
Figures
References
-
- Dvorak HF. Tumors: wounds that do not heal. Similarities between tumor stroma generation and wound healing. N Engl J Med. 1986;315:1650–9. - PubMed
-
- Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357:539–45. - PubMed
-
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454:436–44. - PubMed
-
- Sun B, Karin M. Inflammation and liver tumorigenesis. Front Med. 2013;7:242–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
