

The use of β2-agonist therapy before hospital attendance for severe asthma exacerbations: a post-hoc analysis
- PMID: 25569185
- PMCID: PMC4532151
- DOI: 10.1038/npjpcrm.2014.99
The use of β2-agonist therapy before hospital attendance for severe asthma exacerbations: a post-hoc analysis
Abstract
Background: Patterns of inhaled β2-agonist therapy use during severe asthma exacerbations before hospital attendance are poorly understood.
Aims: To assess β2-agonist use prior to hospital attendance.
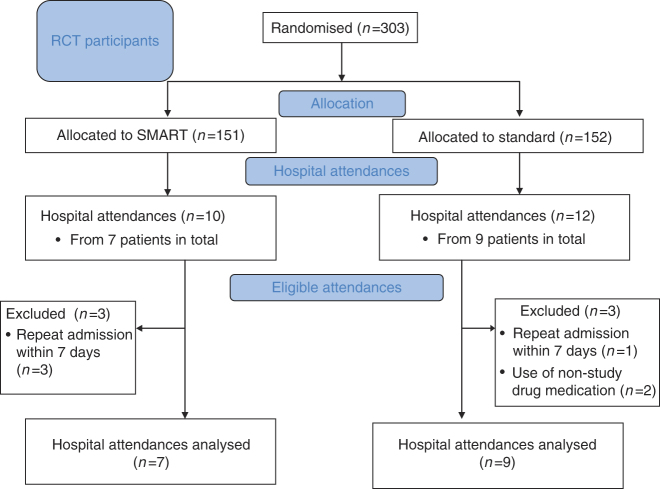
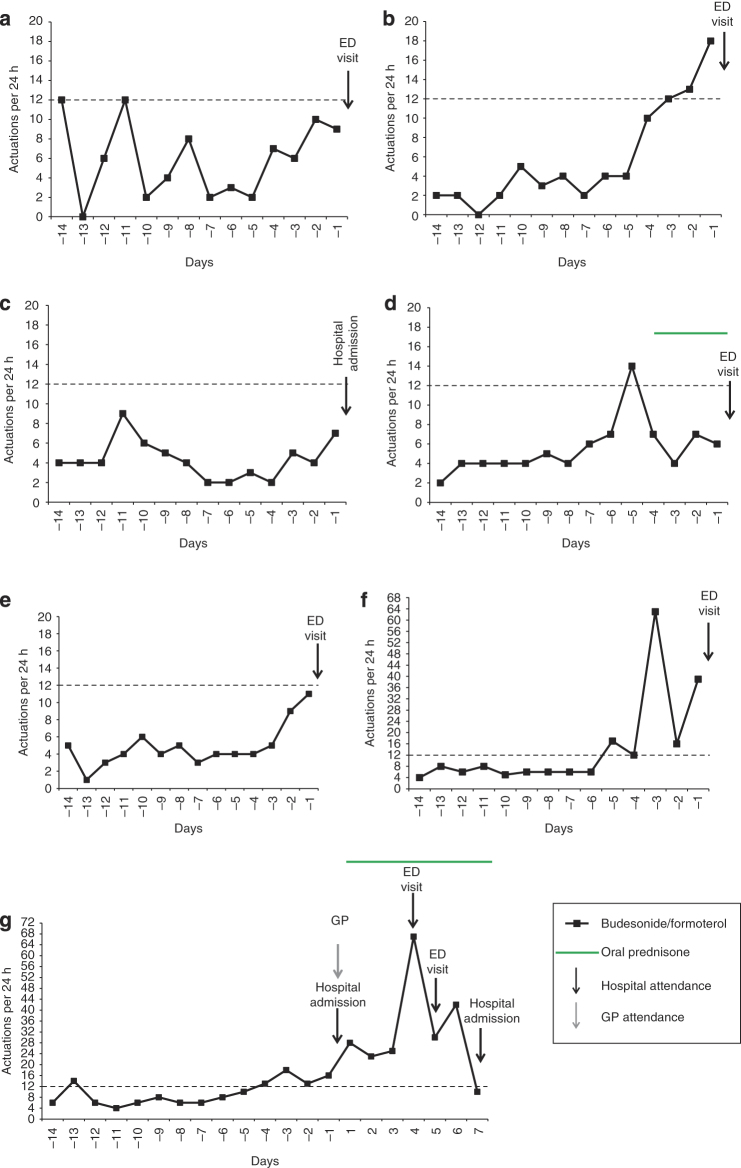
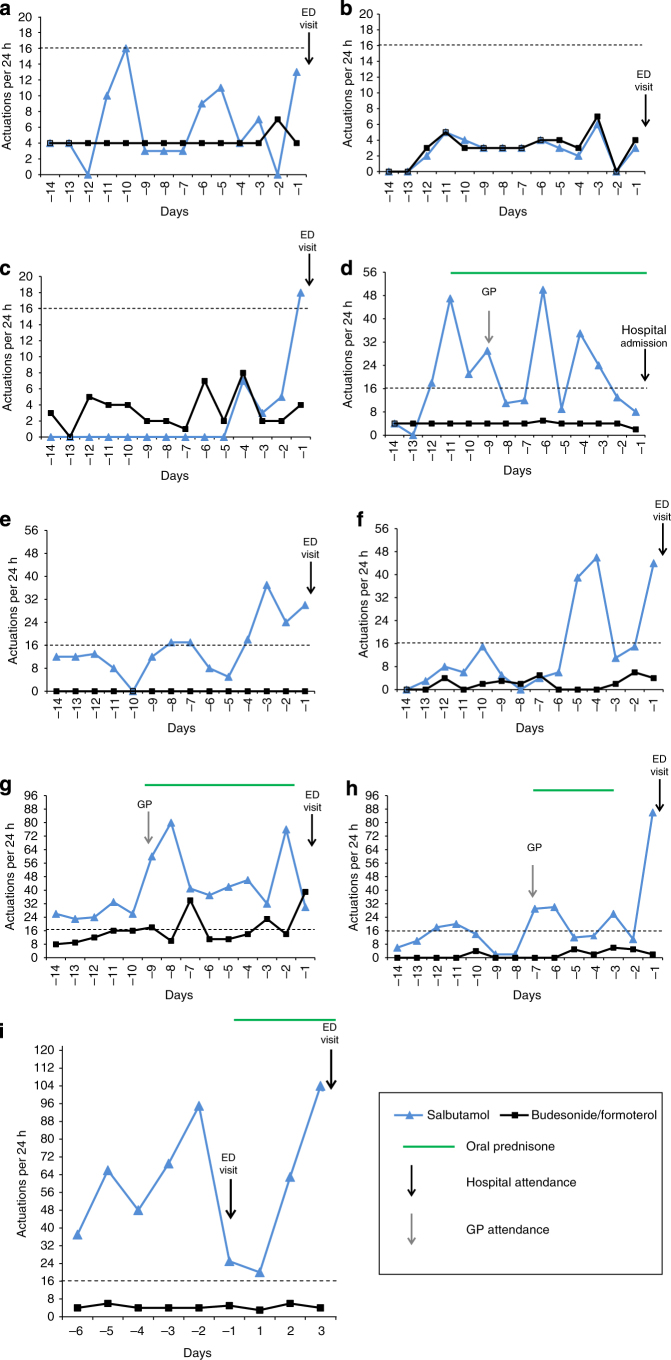
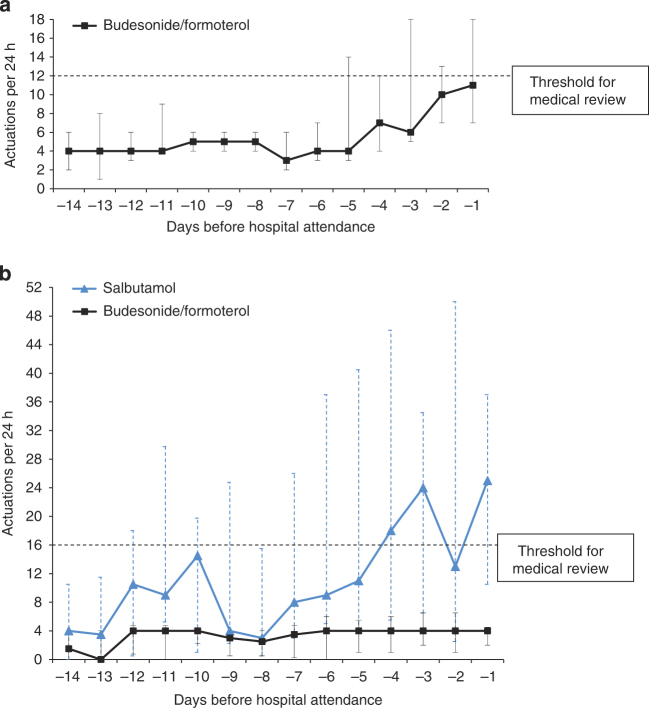
Methods: We undertook an exploratory post hoc analysis of data from a 6-month clinical trial of 303 patients randomised to combination budesonide/formoterol inhaler according to a Single combination inhaler as Maintenance And Reliever Therapy regimen ('SMART') or fixed-dose budesonide/formoterol with salbutamol as reliever ('Standard'). Patterns of β2-agonist use for 14 days before hospital attendance with a severe asthma exacerbation were determined by electronic monitoring of inhaler use.
Results: There were 22 hospital attendances in 16 patients during the study. Seven and nine hospital attendances were eligible for analysis in the SMART and Standard groups, respectively. In both regimens, β2-agonist use increased before hospital attendance, with a median (range) maximum daily number of actuations of 14 (9 to 63) budesonide/formoterol in SMART and 46 (6 to 95) salbutamol in Standard with 4 (0 to 10) budesonide/formoterol actuations on the day of maximal salbutamol use. There was delay in obtaining medical review despite high β2-agonist use, in 9/16 patients. Different patterns of use were observed, including repeated days of no inhaled corticosteroid despite marked salbutamol use, which occurred in 3/9 patients in the Standard group.
Conclusions: Delay in obtaining medical review in association with high β2-agonist use is common in patients before hospital presentation with severe exacerbations of asthma. The SMART regimen reduced nonadherence with inhaled corticosteroid therapy during severe exacerbations.
Figures
Comment in
-
Asthma attacks: how can we reduce the risks?NPJ Prim Care Respir Med. 2015 Jan 8;25:14105. doi: 10.1038/npjpcrm.2014.105. NPJ Prim Care Respir Med. 2015. PMID: 25569849 Free PMC article. No abstract available.
References
-
- Fraser PM, Speizer FE, Waters SD, Doll R, Mann NM. The circumstances preceding death from asthma in young people in 1968 to 1969. Br J Dis Chest. 1971;65:71–84. - PubMed
-
- Sears MR, Rea HH. Patients at risk for dying of asthma: New Zealand experience. J Allergy Clin Immunol. 1987;80:477–481. - PubMed
-
- Beasley R, Pearce N, Crane J, Burgess C. Beta-agonists: what is the evidence that their use increases the risk of asthma morbidity and mortality? J Allergy Clin Immunol. 1999;104:S18–S30. - PubMed
-
- Beasley R, Pearce N, Crane J, Windom H, Burgess C. Asthma mortality and inhaled beta agonist therapy. Aust N Z J Med. 1991;21:753–763. - PubMed
-
- Royal College of Physicians . Why asthma kills: the National Review of Asthma Deaths (NRAD) Confidential Enquiry Report. RCP: London, UK; 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
