

Trends in sepsis and infection sources in the United States. A population-based study
- PMID: 25569845
- PMCID: PMC4342831
- DOI: 10.1513/AnnalsATS.201411-498BC
Trends in sepsis and infection sources in the United States. A population-based study
Abstract
Rationale: Stakeholders seek to monitor processes and outcomes of care among patients with sepsis, but use of administrative data for sepsis surveillance is controversial. Prior studies using only principal diagnoses from claims data have shown a trend of rising sepsis incidence with falling infection incidence, implying that administrative data are inaccurate for sepsis surveillance.
Objectives: Because a sepsis diagnosis often modifies an infection site diagnosis, we sought to investigate trends in sepsis and infection using both principal and secondary diagnoses in administrative data.
Methods: This was a retrospective cohort study. We used data from the Nationwide Inpatient Sample years 2003 to 2009 to identify age-standardized, population-based trends in sepsis and infection using all available diagnosis codes. Infection sites were defined as bacteremia, pneumonia, urinary tract, skin/soft tissue, and gastrointestinal; codes for septicemia, sepsis, severe sepsis, and septic shock were used to identify "sepsis." We identified patients with infection and mechanical ventilation to estimate incidence of severe sepsis without requiring specific claims for sepsis or acute organ failure.
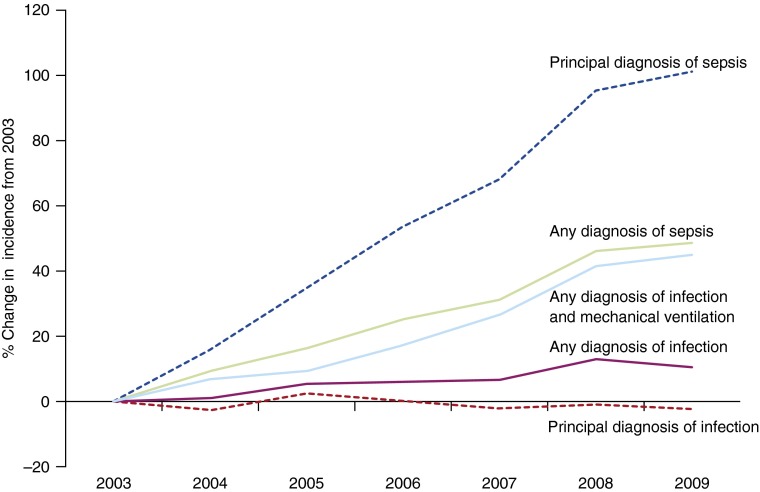
Measurements and main results: We identified 53.9 million adult infection hospitalizations during the years 2003 to 2009; average age was 63 years, 61% of patients were women, and 70% reported white race, 14% black, and 11% Hispanic ethnicity. Incidence of hospitalizations with an infection claim increased from 3,147/100,000 U.S. residents in 2003 to 3,480/100,000 in 2009 (11% increase), whereas hospitalizations with sepsis claims increased from 359/100,000 to 535/100,000 residents during the same time frame (49% increase); P = 0.009 between infection and sepsis trends. The proportion of infection hospitalizations with a sepsis claim increased from 7.5% in 2003 to 11.5% in 2009 (54% increase). The incidence of hospitalizations with both an infection and mechanical ventilation claim during 2003 was 173/100,000 as compared with 251/100,000 in 2009 (45% increase); P = 0.76 compared with sepsis trends.
Conclusions: Sepsis claims are increasing at a greater rate than infection claims but are not inversely related. Trends in sepsis are similar to trends in infection cases requiring mechanical ventilation. Further studies should seek to identify the optimal algorithms to identify sepsis within administrative data and explore potential mechanisms for the increasing incidence of infection and sepsis in the United States.
Keywords: health services research; sepsis.
Figures
Comment in
-
Trends in sepsis and infection sources in the United States. A population-based study.Ann Am Thorac Soc. 2015 May;12(5):784. doi: 10.1513/AnnalsATS.201501-044LE. Ann Am Thorac Soc. 2015. PMID: 25965543 Free PMC article. No abstract available.
-
Reply: trends in sepsis and infection sources in the United States. A population-based study.Ann Am Thorac Soc. 2015 May;12(5):785. doi: 10.1513/AnnalsATS.201503-158LE. Ann Am Thorac Soc. 2015. PMID: 25965544 Free PMC article. No abstract available.
References
-
- Kumar G, Kumar N, Taneja A, Kaleekal T, Tarima S, McGinley E, Jimenez E, Mohan A, Khan RA, Whittle J, et al. Milwaukee Initiative in Critical Care Outcomes Research Group of Investigators. Nationwide trends of severe sepsis in the 21st century (2000-2007) Chest. 2011;140:1223–1231. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007;35:1244–1250. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
