

Ablation of atrial fibrillation
- PMID: 25572010
- PMCID: PMC4764083
- DOI: 10.1016/j.tcm.2014.11.009
Ablation of atrial fibrillation
Abstract
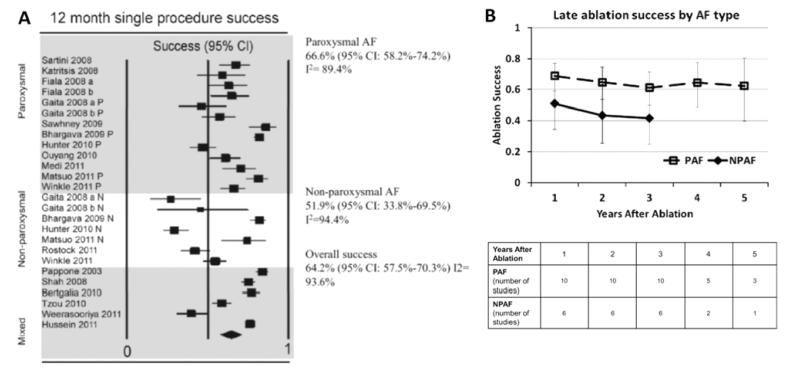
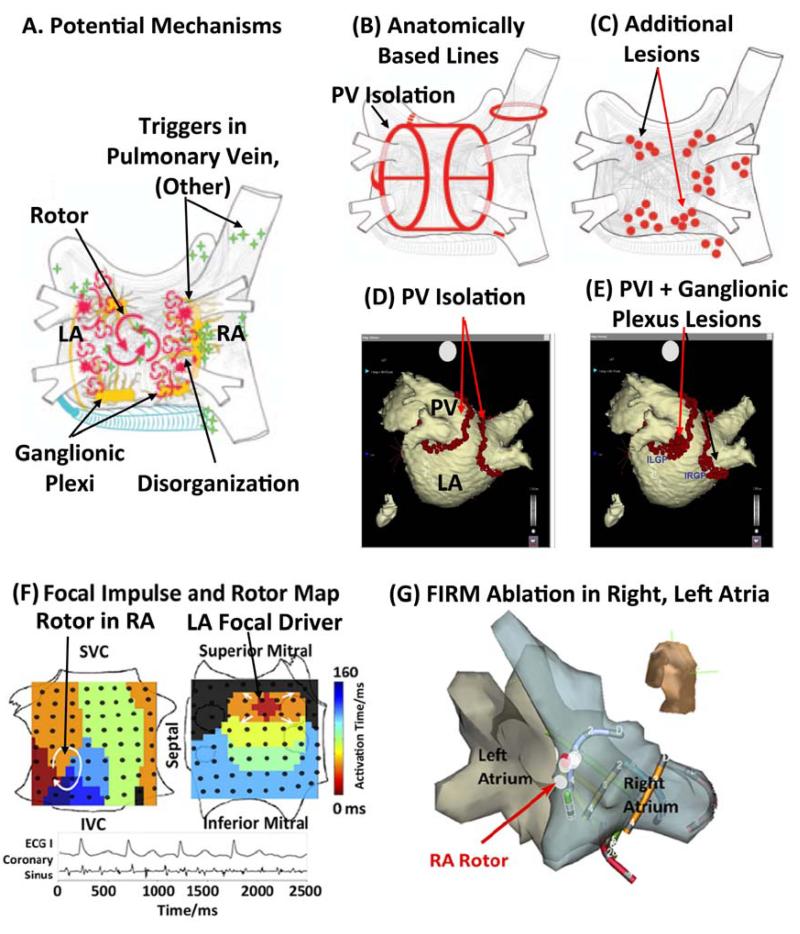
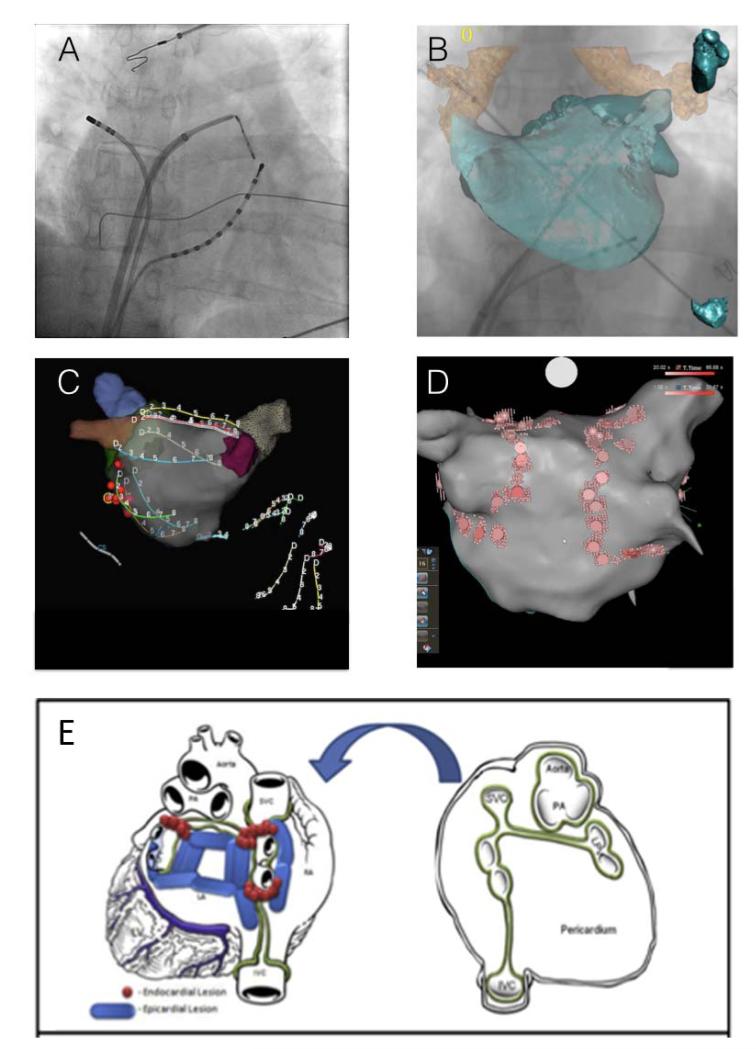
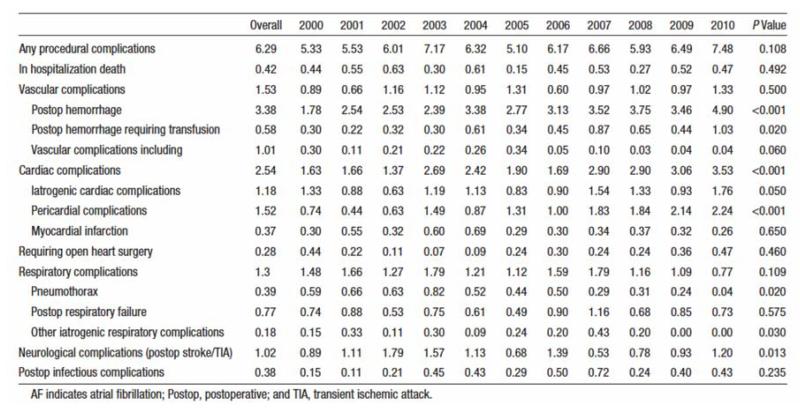
Ablation is increasingly used to treat AF, since recent trials of pharmacological therapy for AF have been disappointing. Ablation has been shown to improve maintenance of sinus rhythm compared to pharmacological therapy in many multicenter trials, although success rates remain suboptimal. This review will discuss several trends in the field of catheter ablation, including studies to advance our understanding of AF mechanisms in different patient populations, innovations in detecting and classifying AF, use of this information to improve strategies for ablation, technical innovations that have improved the ease and safety of ablation, and novel approaches to surgical therapy and imaging. These trends are likely to further improve results from AF ablation in coming years as it becomes an increasingly important therapeutic option for many patients.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Time to switch trains? AF ablation at a pivotal time point.Trends Cardiovasc Med. 2015 Jul;25(5):420-1. doi: 10.1016/j.tcm.2014.11.014. Epub 2014 Dec 4. Trends Cardiovasc Med. 2015. PMID: 25622861 No abstract available.
Similar articles
-
Atrial fibrillation: cure or treat?Ther Adv Cardiovasc Dis. 2009 Jun;3(3):187-96. doi: 10.1177/1753944709104495. Epub 2009 May 14. Ther Adv Cardiovasc Dis. 2009. PMID: 19443515 Review.
-
Catheter ablation is established as a treatment option for atrial fibrillation--is catheter ablation established as a treatment option of atrial fibrillation? (Pro).Circ J. 2010 Sep;74(9):1972-7. doi: 10.1253/circj.cj-10-0693. Epub 2010 Aug 12. Circ J. 2010. PMID: 20716832
-
Catheter Ablation of Atrial Fibrillation in U.S. Community Practice--Results From Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF).J Am Heart Assoc. 2015 May 21;4(5):e001901. doi: 10.1161/JAHA.115.001901. J Am Heart Assoc. 2015. PMID: 25999401 Free PMC article. Clinical Trial.
-
Staged transthoracic approach to persistent atrial fibrillation (TOP-AF): study protocol for a randomized trial.Trials. 2014 May 26;15:190. doi: 10.1186/1745-6215-15-190. Trials. 2014. PMID: 24885377 Free PMC article. Clinical Trial.
-
Improving ablation strategies for the treatment of atrial fibrillation.Expert Rev Med Devices. 2014 Jan;11(1):77-88. doi: 10.1586/17434440.2014.864232. Epub 2013 Dec 2. Expert Rev Med Devices. 2014. PMID: 24308741 Review.
Cited by
-
Novel therapeutic strategies targeting fibroblasts and fibrosis in heart disease.Nat Rev Drug Discov. 2016 Sep;15(9):620-638. doi: 10.1038/nrd.2016.89. Epub 2016 Jun 24. Nat Rev Drug Discov. 2016. PMID: 27339799 Free PMC article. Review.
-
Making better scar: Emerging approaches for modifying mechanical and electrical properties following infarction and ablation.Prog Biophys Mol Biol. 2016 Jan;120(1-3):134-48. doi: 10.1016/j.pbiomolbio.2015.11.002. Epub 2015 Nov 23. Prog Biophys Mol Biol. 2016. PMID: 26615948 Free PMC article. Review.
-
Atrial fibrillation driver mechanisms: Insight from the isolated human heart.Trends Cardiovasc Med. 2017 Jan;27(1):1-11. doi: 10.1016/j.tcm.2016.05.008. Epub 2016 May 24. Trends Cardiovasc Med. 2017. PMID: 27492815 Free PMC article. Review.
References
-
- Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, et al. Lenient versus strict rate control in patients with atrial fibrillation. The New England journal of medicine. 2010;362:1363–73. - PubMed
-
- Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, et al. Rhythm control versus rate control for atrial fibrillation and heart failure. The New England journal of medicine. 2008;358:2667–77. - PubMed
-
- Saksena S, Slee A, Waldo AL, Freemantle N, Reynolds M, Rosenberg Y, et al. Cardiovascular outcomes in the AFFIRM Trial (Atrial Fibrillation Follow-Up Investigation of Rhythm Management). An assessment of individual antiarrhythmic drug therapies compared with rate control with propensity score-matched analyses. J Am Coll Cardiol. 2011;58:1975–85. - PMC - PubMed
-
- Deshmukh A, Patel NJ, Pant S, Shah N, Chothani A, Mehta K, et al. In-hospital complications associated with catheter ablation of atrial fibrillation in the United States between 2000 and 2010: analysis of 93 801 procedures. Circulation. 2013;128:2104–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
