

Costs associated with health care-associated infections in cardiac surgery
- PMID: 25572505
- PMCID: PMC4293042
- DOI: 10.1016/j.jacc.2014.09.079
Costs associated with health care-associated infections in cardiac surgery
Abstract
Background: Health care-associated infections (HAIs) are the most common noncardiac complications after cardiac surgery and are associated with increased morbidity and mortality. Current information about their economic burden is limited.
Objectives: This research was designed to determine the cost associated with major types of HAIs during the first 2 months after cardiac surgery.
Methods: Prospectively collected data from a multicenter, observational study of the Cardiothoracic Surgery Clinical Trials Network, in which patients were monitored for infections for 65 days after surgery, were merged with related financial data routinely collected by the University HealthSystem Consortium. Incremental length of stay (LOS) and cost associated with HAIs were estimated using generalized linear models, with adjustments for patient demographics, clinical history, baseline laboratory values, and surgery type.
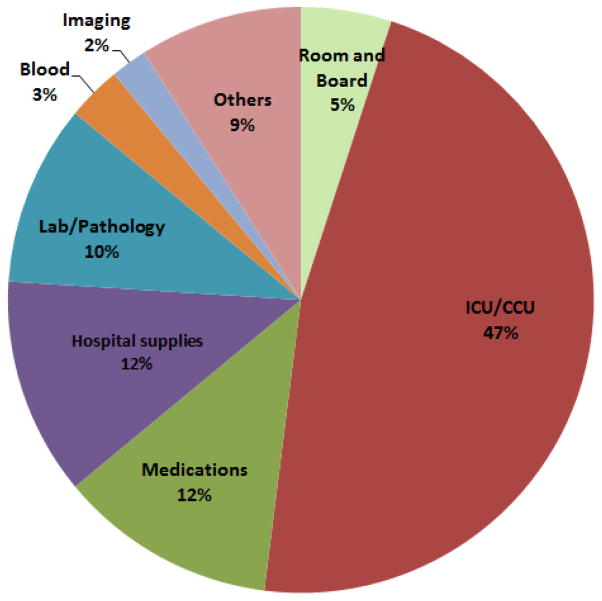
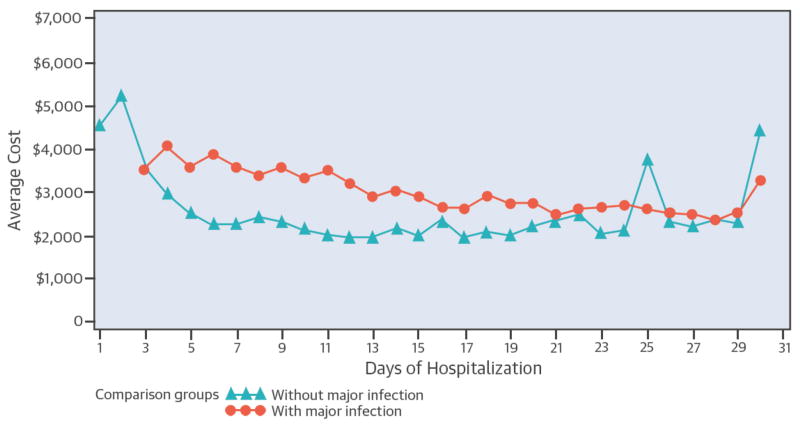
Results: Among 4,320 cardiac surgery patients (mean age: 64 ± 13 years), 119 (2.8%) experienced a major HAI during the index hospitalization. The most common HAIs were pneumonia (48%), sepsis (20%), and Clostridium difficile colitis (18%). On average, the estimated incremental cost associated with a major HAI was nearly $38,000, of which 47% was related to intensive care unit services. The incremental LOS was 14 days. Overall, there were 849 readmissions; among these, 8.7% were attributed to major HAIs. The cost of readmissions due to major HAIs was, on average, nearly threefold that of readmissions not related to HAIs.
Conclusions: Hospital cost, LOS, and readmissions are strongly associated with HAIs. These associations suggest the potential for large reductions in costs if HAIs following cardiac surgery can be reduced. (Management Practices and the Risk of Infections Following Cardiac Surgery; NCT01089712).
Keywords: health care–associated infection; hospital costs; length of stay.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Infections following cardiac surgery: an opportunity for clarity.J Am Coll Cardiol. 2015 Jan 6;65(1):24-26. doi: 10.1016/j.jacc.2014.10.028. J Am Coll Cardiol. 2015. PMID: 25572506 No abstract available.
References
-
- Ridderstolpe L, Gill H, Granfeldt H, Ahlfeldt H, Rutberg H. Superficial and deep sternal wound complications: incidence, risk factors and mortality. European journal of cardio-thoracic surgery: official journal of the European Association for Cardio-thoracic Surgery. 2001;20:1168–75. - PubMed
-
- Fowler VG, Jr, O’Brien SM, Muhlbaier LH, Corey GR, Ferguson TB, Peterson ED. Clinical predictors of major infections after cardiac surgery. Circulation. 2005;112:I358–65. - PubMed
-
- Edwards FH, Ferguson TB. The Society of Thoracic Surgeons Practice Guidelines. Ann Thorac Surg. 2004;77:1140–1. - PubMed
-
- Kollef MH, Sharpless L, Vlasnik J, Pasque C, Murphy D, Fraser VJ. The impact of nosocomial infections on patient outcomes following cardiac surgery. Chest. 1997;112:666–75. - PubMed
-
- Brown PP, Kugelmass AD, Cohen DJ, et al. The frequency and cost of complications associated with coronary artery bypass grafting surgery: results from the United States Medicare program. Ann Thorac Surg. 2008;85:1980–6. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
