

Metabolite profiling and cardiovascular event risk: a prospective study of 3 population-based cohorts
- PMID: 25573147
- PMCID: PMC4351161
- DOI: 10.1161/CIRCULATIONAHA.114.013116
Metabolite profiling and cardiovascular event risk: a prospective study of 3 population-based cohorts
Abstract
Background: High-throughput profiling of circulating metabolites may improve cardiovascular risk prediction over established risk factors.
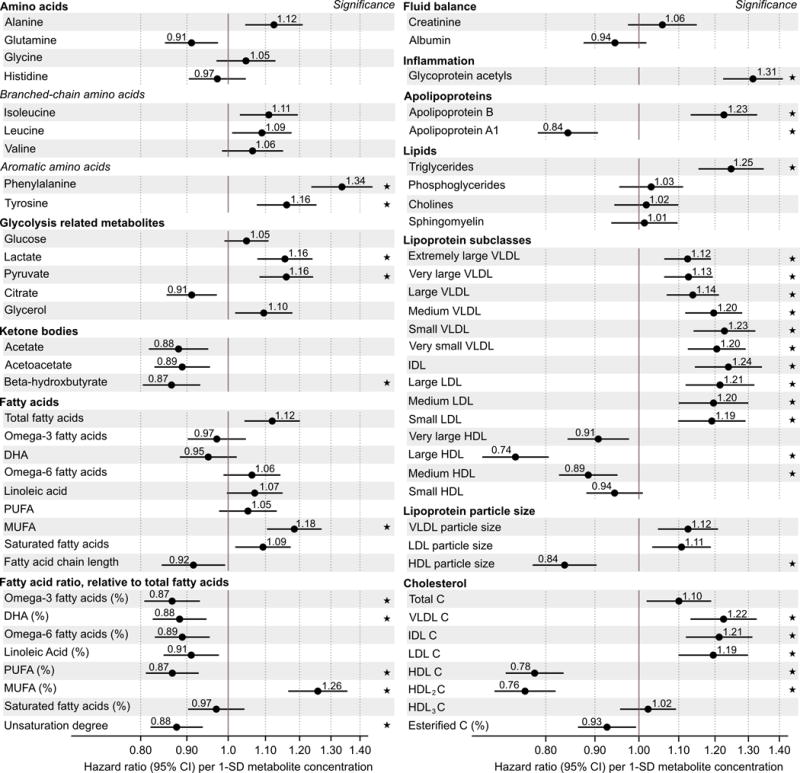
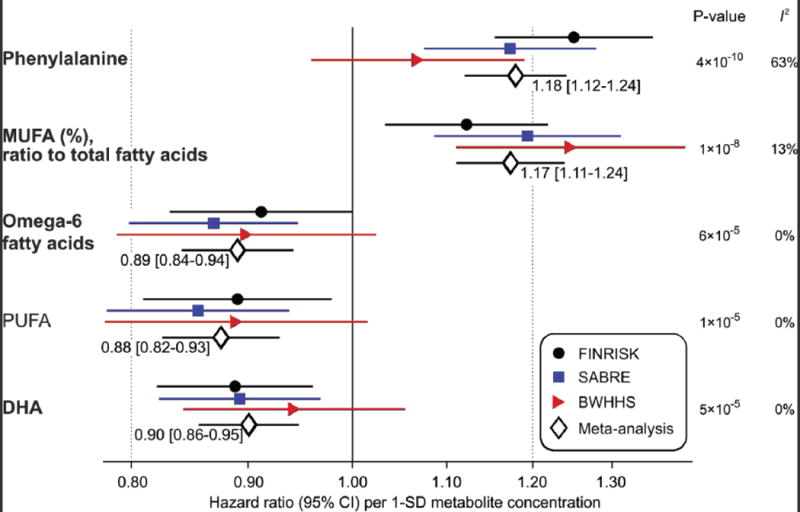
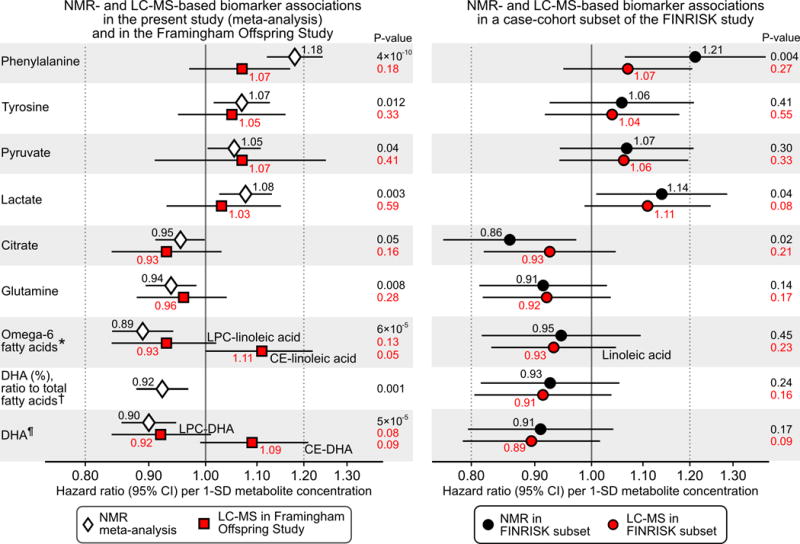
Methods and results: We applied quantitative nuclear magnetic resonance metabolomics to identify the biomarkers for incident cardiovascular disease during long-term follow-up. Biomarker discovery was conducted in the National Finnish FINRISK study (n=7256; 800 events). Replication and incremental risk prediction was assessed in the Southall and Brent Revisited (SABRE) study (n=2622; 573 events) and British Women's Health and Heart Study (n=3563; 368 events). In targeted analyses of 68 lipids and metabolites, 33 measures were associated with incident cardiovascular events at P<0.0007 after adjusting for age, sex, blood pressure, smoking, diabetes mellitus, and medication. When further adjusting for routine lipids, 4 metabolites were associated with future cardiovascular events in meta-analyses: higher serum phenylalanine (hazard ratio per standard deviation, 1.18; 95% confidence interval, 1.12-1.24; P=4×10(-10)) and monounsaturated fatty acid levels (1.17; 1.11-1.24; P=1×10(-8)) were associated with increased cardiovascular risk, while higher omega-6 fatty acids (0.89; 0.84-0.94; P=6×10(-5)) and docosahexaenoic acid levels (0.90; 0.86-0.95; P=5×10(-5)) were associated with lower risk. A risk score incorporating these 4 biomarkers was derived in FINRISK. Risk prediction estimates were more accurate in the 2 validation cohorts (relative integrated discrimination improvement, 8.8% and 4.3%), albeit discrimination was not enhanced. Risk classification was particularly improved for persons in the 5% to 10% risk range (net reclassification, 27.1% and 15.5%). Biomarker associations were further corroborated with mass spectrometry in FINRISK (n=671) and the Framingham Offspring Study (n=2289).
Conclusions: Metabolite profiling in large prospective cohorts identified phenylalanine, monounsaturated fatty acids, and polyunsaturated fatty acids as biomarkers for cardiovascular risk. This study substantiates the value of high-throughput metabolomics for biomarker discovery and improved risk assessment.
Keywords: amino acids; biological markers; fatty acids; metabolomics; risk factors.
© 2015 American Heart Association, Inc.
Figures

References
-
- Lloyd-Jones DM. Cardiovascular risk prediction: basic concepts, current status, and future directions. Circulation. 2010;121:1768–1777. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC, Jr, Watson K, Wilson PW, Eddleman KM, Jarrett NM, LaBresh K, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC, Jr, Tomaselli GF. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–45. - PubMed
-
- NICE clinical guideline 181. Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. 2014 Jul; guidance.nice.org.uk/cg181. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- SP/07/001/23603/BHF_/British Heart Foundation/United Kingdom
- R01 DK 081572/DK/NIDDK NIH HHS/United States
- PG/13/66/30442/BHF_/British Heart Foundation/United Kingdom
- CS/13/1/30327/BHF_/British Heart Foundation/United Kingdom
- PG/08/103/26133/BHF_/British Heart Foundation/United Kingdom
- WT082464AIA/WT_/Wellcome Trust/United Kingdom
- PG/12/29/29497/BHF_/British Heart Foundation/United Kingdom
- N01 HC025195/HL/NHLBI NIH HHS/United States
- G1000427/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- R01 HL98280/HL/NHLBI NIH HHS/United States
- MC_UU_12013/5/MRC_/Medical Research Council/United Kingdom
- MC_UU_12013/8/MRC_/Medical Research Council/United Kingdom
- R01 DK081572/DK/NIDDK NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- R01 HL098280/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
