

Reducing CKD risks among vulnerable populations in primary care
- PMID: 25573516
- PMCID: PMC4291538
- DOI: 10.1053/j.ackd.2014.06.003
Reducing CKD risks among vulnerable populations in primary care
Abstract
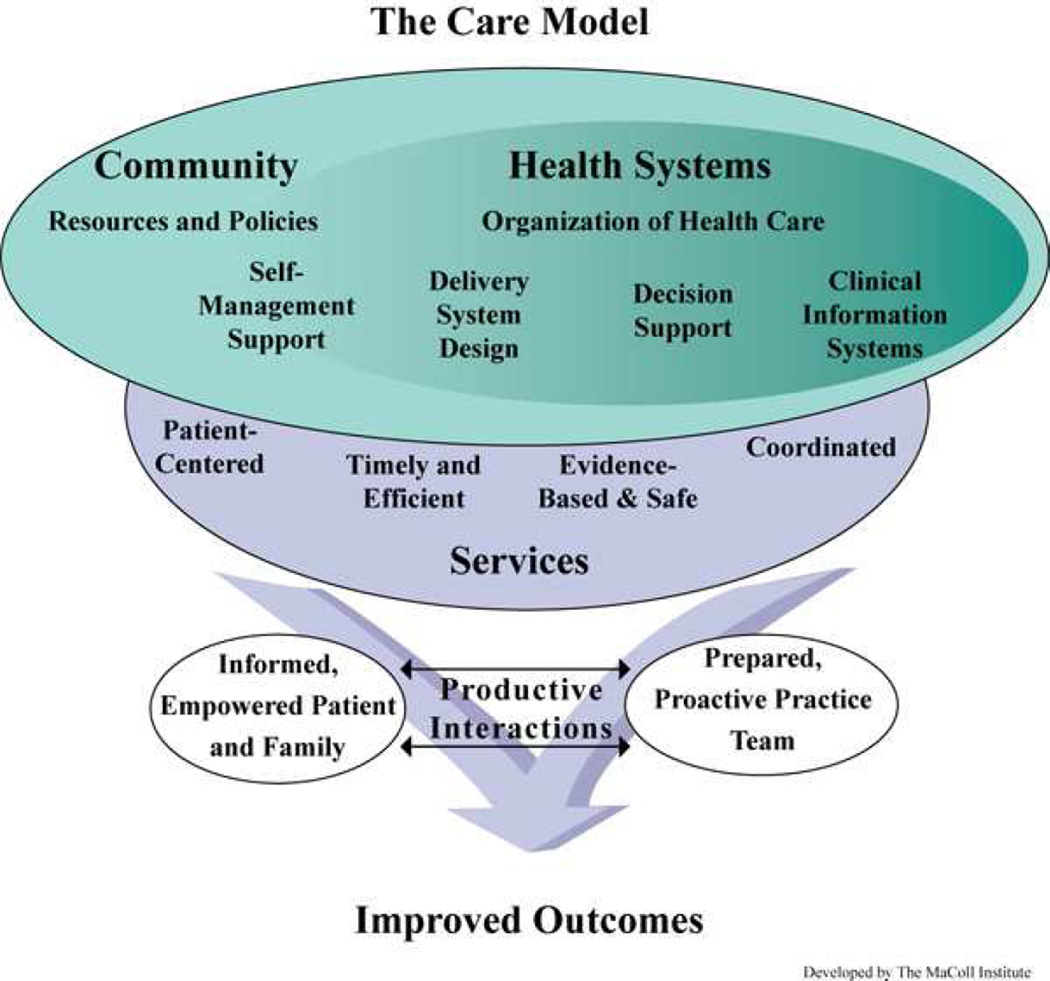
Ethnic/racial and socioeconomic status disparities in the health-care and clinical outcomes of patients with chronic kidney disease (CKD) are pervasive. The vast majority of care to decrease incidence of CKD risk and progression occurs in primary care settings. High-quality primary care, therefore, represents a key strategy through which disparities in the incidence and progression of CKD may be eliminated. The Chronic Care Model provides a framework for the delivery of high-quality primary care for chronic diseases, and it is frequently used to guide health-care quality improvement initiatives. Evidence suggests that Chronic Care Model constructs, including provider and organizational quality improvement initiatives focused on team approaches to chronic care (eg, case management, community health workers), are effective in modifying patients' CKD risks among ethnic minority and low-income patients. Other Chronic Care Model constructs, including clinical information systems (eg, disease registries), decision support interventions, and the provision of patient-centered care have been shown to improve processes related to CKD care but with limited and/or mixed effects on patient outcomes. Few studies have examined the effect of these approaches on reducing disparities. Research is needed to examine the effectiveness of these strategies to eliminate CKD disparities among vulnerable populations.
Keywords: Chronic kidney disease; Health-care disparities; Primary care; Quality improvement; Socioeconomic status.
Copyright © 2015 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial Closure Statement: The authors have no financial conflicts of interests.
Figures
References
-
- Tarver-Carr ME, Powe NR, Eberhardt MS, et al. Excess risk of chronic kidney disease among African-American versus white subjects in the United States: a population-based study of potential explanatory factors. J Am Soc Nephrol. 2002;13:2363–2370. - PubMed
-
- Li S, McAlpine DD, Liu J, Collins AJ. Differences between blacks and whites in the incidence of end-stage renal disease and associated risk factors. Adv Ren Replace Ther. 2004;11:5–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
