

Additional bone graft accelerates healing of clavicle non-unions and improves long-term results after 8.9 years: a retrospective study
- PMID: 25573541
- PMCID: PMC4296679
- DOI: 10.1186/s13018-014-0143-y
Additional bone graft accelerates healing of clavicle non-unions and improves long-term results after 8.9 years: a retrospective study
Abstract
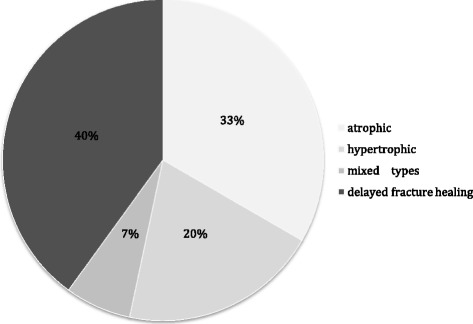
Background: Clavicle non-unions can occur after both conservative and operative treatment failure. Here, we investigated the outcome of patients with delayed fracture healing or non-unions of the clavicle. Patients underwent revision surgery by plate osteosynthesis of the clavicle with or without bone grafting. Our aim was to determine rates of bone healing and the functional long-term outcome.
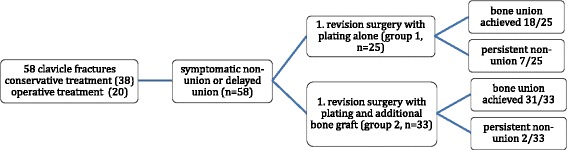
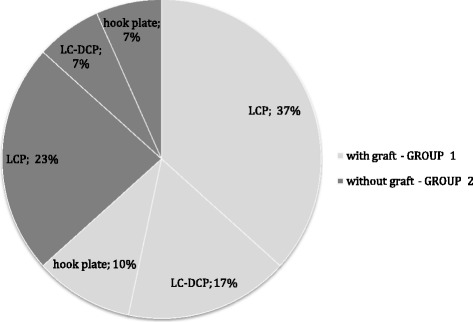
Methods: The study population of 58 consecutive patients was divided into group 1 (n = 25; no bone graft) and group 2 (n = 33; iliac crest bone graft). Bone consolidation was determined by the Lane-Sandhu score preoperatively and after 2.2 ± 1.8 years, respectively. The functional long-term outcome was determined after 8.9 ± 2.7 years in all available patients (n = 30) by the Constant score, DASH (Disabilities of the Arm, Shoulder and Hand) score and SF-36, and clavicle length was measured by ultrasound as compared to the healthy side.
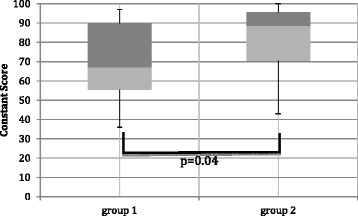
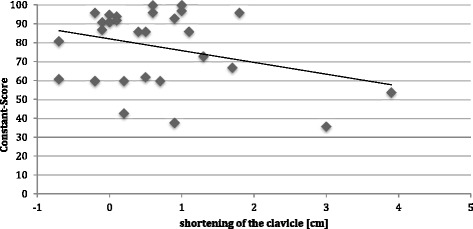
Results: Clavicle consolidation was achieved in 54 out of 58 patients (93.1%) after revision surgeries. The radiographic score and bone consolidation rates were significantly higher in group 2 (93.3%) as compared with 72% in group 1 (p = 0.02), resulting in a significantly shorter time to bone consolidation in group 2. Similarly, the relative risk for additional surgery after the first revision surgery was 4.7-fold higher in group 1 (p = 0.02). The long-term results showed overall very good results in DASH score (14.9 ± 16.5) and good results in Constant scores (77.9 ± 19.9). The group analyses found significantly better Constant scores and better visual analogue pain scale (VAS) numbers in group 2. Clavicle shortening appeared to affect the clinical results, and a mild correlation between shortening and Constant scores (R = -0.31) was found.
Conclusions: This study shows high rates of bone healing and good functional outcomes after surgical revision of clavicle non-unions and further demonstrates that additional bone graft could significantly accelerate bone healing. This indicates that revision surgery of clavicle non-unions might preferably be done with additional bone graft, even if the surgeon considers that bone healing might be achieved without bone grafting.
Figures
References
-
- Lenza M, Buchbinder R, Johnston RV, Belloti JC, Faloppa F. Surgical versus conservative interventions for treating fractures of the middle third of the clavicle. The Cochrane database of Syst Rev. 2013;6:CD009363. - PubMed
-
- Kraus TM, Martetschlager F, Schrodl C, Siebenlist S, Ganslmeier A, Kirchhoff C, et al. Elastic stable intramedullary nailing of clavicular midshaft fractures: comparison of open vs closed fracture reduction. Der Unfallchirurg. 2013;102:104–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
