

Cigarette smoking and cardiovascular events: role of inflammation and subclinical atherosclerosis from the MultiEthnic Study of Atherosclerosis
- PMID: 25573855
- PMCID: PMC4404404
- DOI: 10.1161/ATVBAHA.114.304562
Cigarette smoking and cardiovascular events: role of inflammation and subclinical atherosclerosis from the MultiEthnic Study of Atherosclerosis
Abstract
Objectives: To examine the contemporary effect of smoking in a multiethnic sample, and to explore the respective contributions of inflammation and subclinical atherosclerosis to the cardiovascular consequences of smoking.
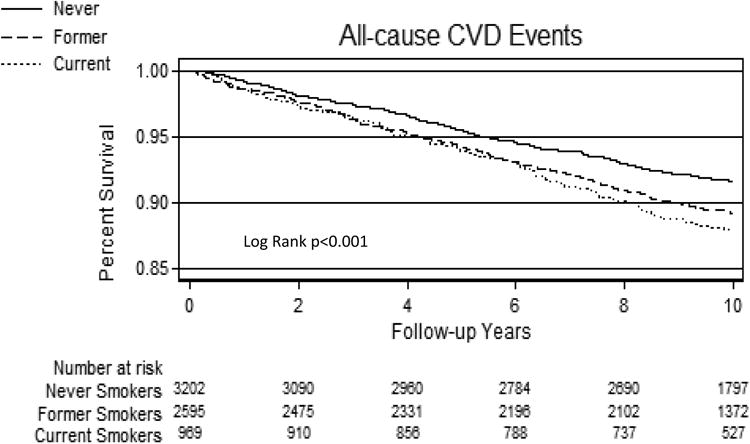
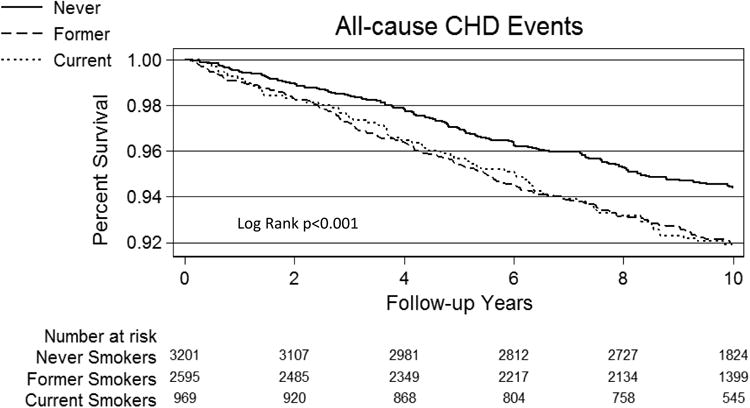
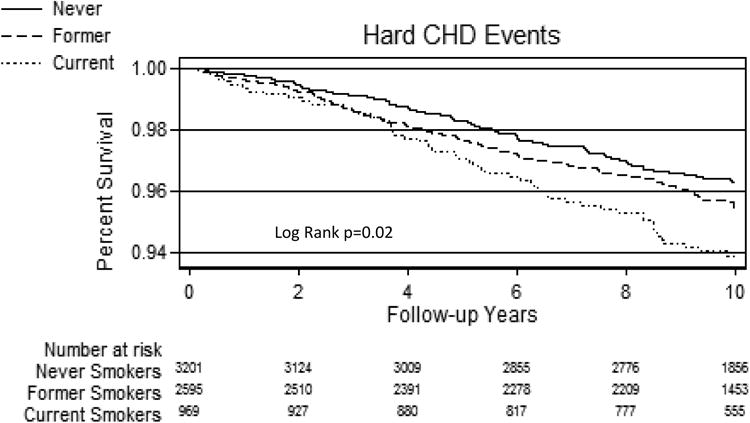
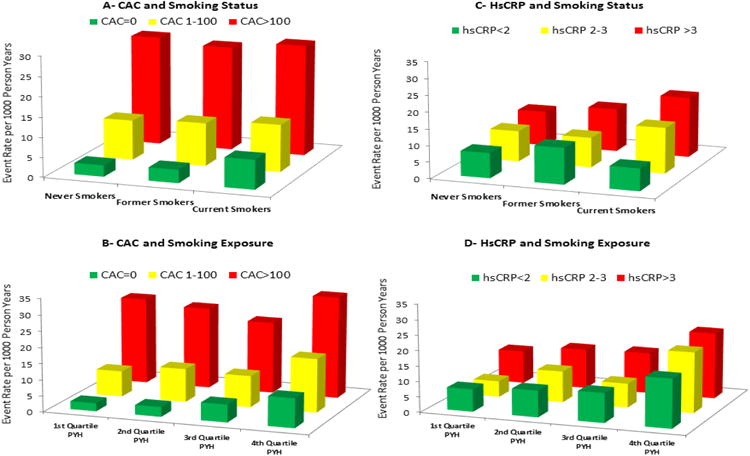
Approach and results: We studied 6814 participants free of cardiovascular disease and coronary heart disease (CHD) from the Multiethnic Study of Atherosclerosis. Smoking status and cumulative exposure were determined by self-report and confirmed by urinary cotinine. Multivariable Cox regression was used to estimate the association between smoking parameters and all-cause cardiovascular disease, all-cause CHD, and hard CHD events. We further adjusted for high-sensitivity C-reactive protein and coronary artery calcium (CAC) in hierarchical Cox models. We identified 3218 never smokers, 2607 former smokers, and 971 current smokers. Median follow-up was 10.2 years. Compared with never smokers, adjusted hazard ratios in current smokers were 1.7 (95% confidence interval, 1.3-2.2) for all-cause cardiovascular disease, 1.6 (1.1-2.1) for all-cause CHD, and 1.7 (1.2-2.4) for hard CHD. Similarly, among current smokers, hazard ratios were higher in the 4th versus 1st quartile of pack-years (eg, all-cause CHD hazard ratio=2.7 [1.1-6.6]). Both CAC>100 and high-sensitivity C-reactive protein ≥3 mg/L identified higher relative risk among current smokers (eg, all-cause CHD hazard ratio of 3.0 [1.5-6.0, compared with CAC=0] and 2.6 [1.4-4.8, compared with high-sensitivity C-reactive protein <2 mg/L], respectively). However, CAC was a stronger mediator of events and adversely modified the effect of smoking on events (eg, P-interaction=0.02 for hard CHD). Compared with never smokers, former smokers (median cessation interval=22 years) had similar adjusted hazard for events.
Conclusions: In this multiethnic cohort, current smoking and cumulative exposure remain important modifiable determinants of cardiovascular disease. Both high-sensitivity C-reactive protein ≥3 mg/L and, particularly, CAC>100 identified high-risk smokers who may benefit from more intensive smoking-cessation efforts.
Keywords: coronary artery disease; inflammation; smoking.
© 2015 American Heart Association, Inc.
Figures
References
-
- Schroeder SA. New evidence that cigarette smoking remains the most important health hazard. The New England journal of medicine. 2013;368:389–390. - PubMed
-
- The health consequences of smoking-50 years of progress: A report of the surgeon general. Atlanta (GA): 2014.
-
- Barua RS, Ambrose JA. Mechanisms of coronary thrombosis in cigarette smoke exposure. Arteriosclerosis, thrombosis, and vascular biology. 2013;33:1460–1467. - PubMed
-
- Hammond EC, Horn D. Smoking and death rates: Report on forty-four months of follow-up of 187,783 men. 2. Death rates by cause. Journal of the American Medical Association. 1958;166:1294–1308. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P50 HL120163/HL/NHLBI NIH HHS/United States
- 1 P50 HL120163-01/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- R01-HL077612/HL/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- U54 HL120163/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
