

Autoimmune hepatitis, one disease with many faces: etiopathogenetic, clinico-laboratory and histological characteristics
- PMID: 25574080
- PMCID: PMC4284362
- DOI: 10.3748/wjg.v21.i1.60
Autoimmune hepatitis, one disease with many faces: etiopathogenetic, clinico-laboratory and histological characteristics
Abstract
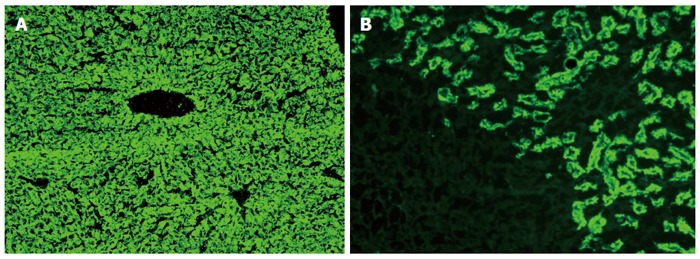
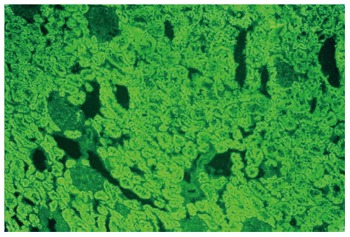
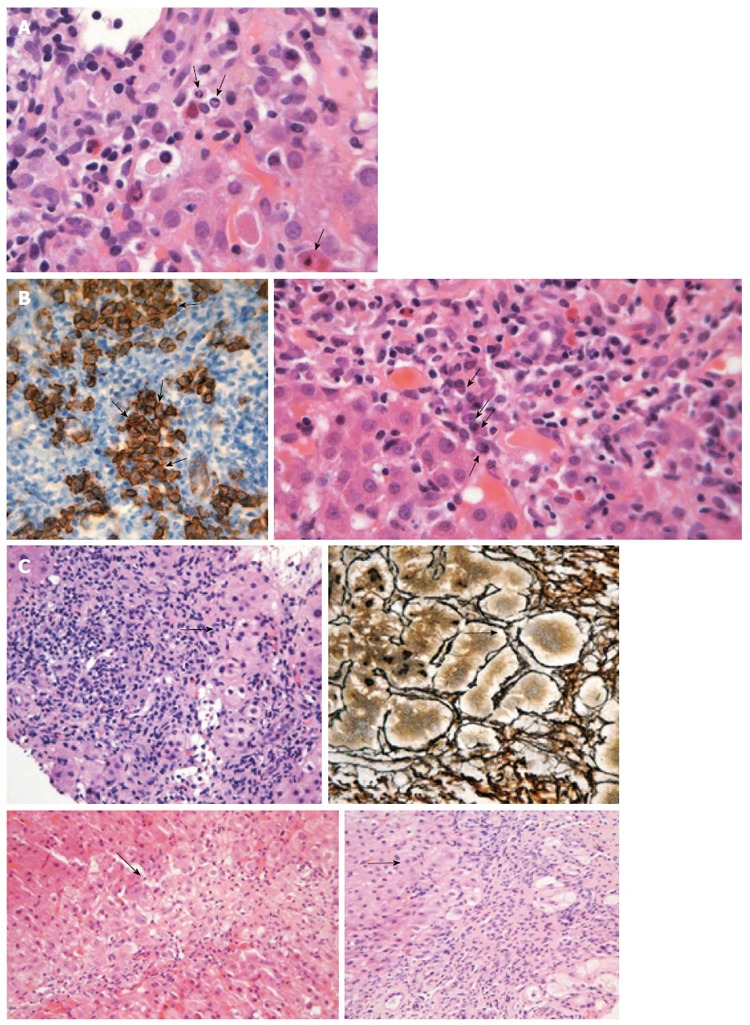
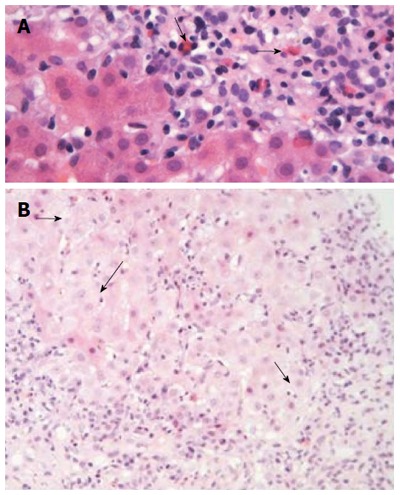
Autoimmune hepatitis (AIH) is an unresolving progressive liver disease of unknown etiology characterized by hypergammaglobulinemia, autoantibodies detection and interface hepatitis. Due to the absence of specific diagnostic markers and the large heterogeneity of its clinical, laboratory and histological features, AIH diagnosis may be potentially difficult. Therefore, in this in-depth review we summarize the substantial progress on etiopathogenesis, clinical, serological and histological phenotypes of AIH. AIH has a global distribution affecting any age, both sexes and all ethnic groups. Clinical manifestations vary from asymptomatic to severe or rarely fulminant hepatitis. Hypergammaglobulinemia with selective elevation of IgG is found in most cases. Autoimmune attack is perpetuated, possibly via molecular mimicry, and favored by the impaired control of T-regulatory cells. Histology (interface hepatitis, emperipolesis and hepatic rosette formation) and autoantibodies detection although not pathognomonic, are still the hallmark for a timely diagnosis. AIH remains a major diagnostic challenge. AIH should be considered in every case in the absence of viral, metabolic, genetic and toxic etiology of chronic or acute hepatitis. Laboratory personnel, hepato-pathologists and clinicians need to become more familiar with disease expressions and the interpretation of liver histology and autoimmune serology to derive maximum benefit for the patient.
Keywords: Autoimmune hepatitis; Liver autoimmunity; Liver-related autoantibodies; Non-organ specific autoantibodies; Overlap syndromes.
Figures
References
-
- Zachou K, Muratori P, Koukoulis GK, Granito A, Gatselis N, Fabbri A, Dalekos GN, Muratori L. Review article: autoimmune hepatitis -- current management and challenges. Aliment Pharmacol Ther. 2013;38:887–913. - PubMed
-
- Dalekos GN, Zachou K, Liaskos C, Gatselis N. Autoantibodies and defined target autoantigens in autoimmune hepatitis: an overview. Eur J Intern Med. 2002;13:293–303. - PubMed
-
- Czaja AJ. Autoantibodies in autoimmune liver disease. Adv Clin Chem. 2005;40:127–164. - PubMed
-
- Krawitt EL. Can you recognize autoimmune hepatitis? Postgrad Med. 1998;104:145–149, 152. - PubMed
-
- Johnson PJ, McFarlane IG. Meeting report: International Autoimmune Hepatitis Group. Hepatology. 1993;18:998–1005. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
