

Post-hepatectomy survival in advanced hepatocellular carcinoma with portal vein tumor thrombosis
- PMID: 25574098
- PMCID: PMC4284342
- DOI: 10.3748/wjg.v21.i1.246
Post-hepatectomy survival in advanced hepatocellular carcinoma with portal vein tumor thrombosis
Abstract
Aim: To analyze hepatocellular carcinoma (HCC) patients with portal vein tumor thrombosis (PVTT) using the tumor-node-metastasis (TNM) staging system.
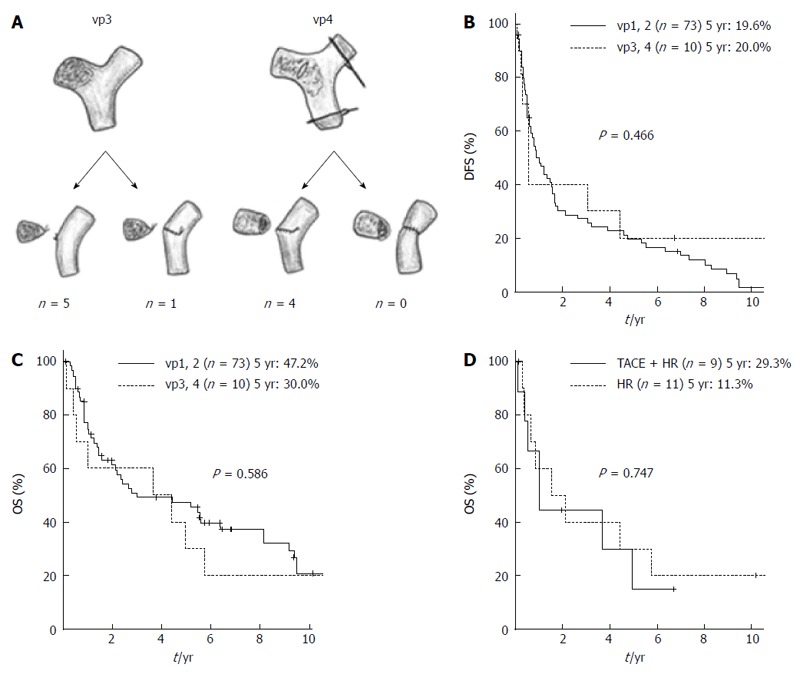
Methods: We retrospectively analyzed 372 patients with HCC who underwent hepatectomy between 1980 and 2009. We studied the outcomes of HCC patients with PVTT to evaluate the American Joint Committee on Cancer TNM staging system (7(th) edition) for stratifying and predicting the prognosis of a large cohort of HCC patients after hepatectomy in a single-center. Portal vein invasion (vp) 1 was defined as an invasion or tumor thrombus distal to the second branch of the portal vein, vp2 as an invasion or tumor thrombus in the second branch of the portal vein, vp3 as an invasion or tumor thrombus in the first branch of the portal vein, and vp4 as an invasion or tumor thrombus in the portal trunk or extending to a branch on the contralateral side.
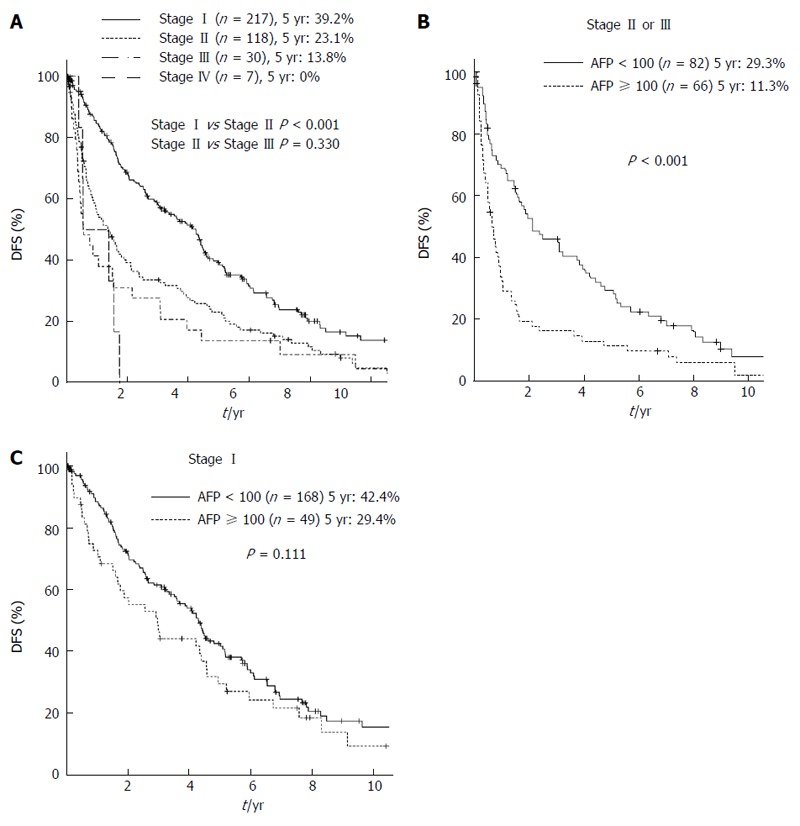
Results: The cumulative 5-year overall survival (5yrOS) and 5-year disease-free survival (5yrDFS) rates of the 372 patients were 58.3% and 31.3%, respectively. The 5yrDFS and 5yrOS of vp3-4 patients (n = 10) were 20.0%, and 30.0%, respectively, which was comparable with the corresponding survival rates of vp1-2 patients (P = 0.466 and 0.586, respectively). In the subgroup analysis of patients with macroscopic PVTT (vp2-4), the OS of the patients who underwent preoperative transarterial chemoembolization was comparable to that of patients who did not (P = 0.747). There was a significant difference in the DFS between patients with stage I HCC and those with stage II HCC (5yrDFS 39.2% vs 23.1%, P < 0.001); however, the DFS for stage II was similar to that for stage III (5yrDFS 23.1% vs 13.8%, P = 0.330). In the subgroup analysis of stage II-III HCC (n = 148), only alpha-fetoprotein (AFP) > 100 mg/dL was independently associated with DFS.
Conclusion: Hepatectomy for vp3-4 HCC results in a survival rate similar to hepatectomy for vp1-2. AFP stratified the stage II-III HCC patients according to prognosis.
Keywords: Alpha-fetoprotein; Hepatectomy; Hepatocellular carcinoma; Portal vein tumor thrombosis; Tumor-node-metastasis staging system.
Figures
References
-
- Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127:S5–S16. - PubMed
-
- Yamamoto Y, Ikoma H, Morimura R, Konishi H, Murayama Y, Komatsu S, Shiozaki A, Kuriu Y, Kubota T, Nakanishi M, et al. Changing trends in long-term outcomes after hepatic resection for hepatocellular carcinoma: A 30-year, single-center experience. Anticancer Res. 2013;33:5097–5105. - PubMed
-
- Izumi R, Shimizu K, Ii T, Yagi M, Matsui O, Nonomura A, Miyazaki I. Prognostic factors of hepatocellular carcinoma in patients undergoing hepatic resection. Gastroenterology. 1994;106:720–727. - PubMed
-
- Ban D, Shimada K, Yamamoto Y, Nara S, Esaki M, Sakamoto Y, Kosuge T. Efficacy of a hepatectomy and a tumor thrombectomy for hepatocellular carcinoma with tumor thrombus extending to the main portal vein. J Gastrointest Surg. 2009;13:1921–1928. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
