

Long-term survival after resection of pancreatic cancer: a single-center retrospective analysis
- PMID: 25574100
- PMCID: PMC4284344
- DOI: 10.3748/wjg.v21.i1.262
Long-term survival after resection of pancreatic cancer: a single-center retrospective analysis
Abstract
Aim: To retrospectively analyze factors affecting the long-term survival of patients with pancreatic cancer who underwent pancreatic resection.
Methods: From January 2000 to December 2011, 195 patients underwent pancreatic resection in our hospital. The prognostic factors after pancreatic resection were analyzed in all 195 patients. After excluding the censored cases within an observational period, the clinicopathological characteristics of 20 patients who survived ≥ 5 (n = 20) and < 5 (n = 76) years were compared. For this comparison, we analyzed the patients who underwent surgery before June 2008 and were observed for more than 5 years. For statistical analyses, the log-rank test was used to compare the cumulative survival rates, and the χ (2) and Mann-Whitney tests were used to compare the two groups. The Cox-Hazard model was used for a multivariate analysis, and P values less than 0.05 were considered significant. A multivariate analysis was conducted on the factors that were significant in the univariate analysis.
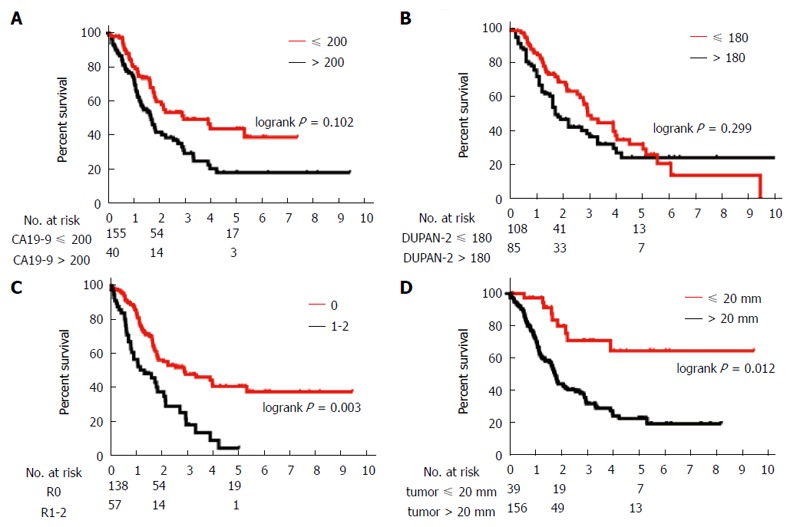
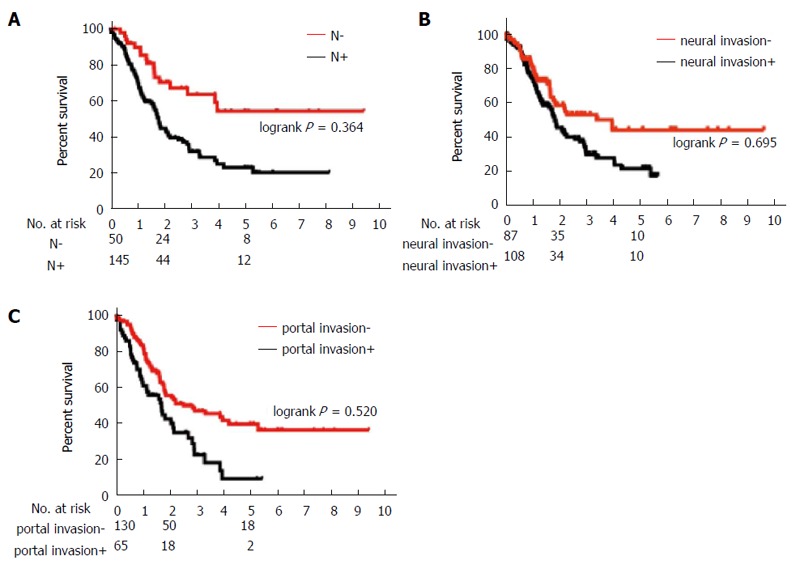
Results: The median survival for all patients was 27.1 months, and the 5-year actuarial survival rate was 34.5%. The median observational period was 595 d. With the univariate analysis, the UICC stage was significantly associated with survival time, and the CA19-9 ≤ 200 U/mL, DUPAN-2 ≤ 180 U/mL, tumor size ≤ 20 mm, R0 resection, absence of lymph node metastasis, absence of extrapancreatic neural invasion, and absence of portal invasion were favorable prognostic factors. The multivariate analysis showed that tumor size ≤ 20 mm (HR = 0.40; 95%CI: 0.17-0.83, P = 0.012) and negative surgical margins (R0 resection) (HR = 0.48; 95%CI: 0.30-0.77, P = 0.003) were independent favorable prognostic factors. Among the 96 patients, 20 patients survived for 5 years or more, and 76 patients died within 5 years after operation. Comparison of the 20 5-year survivors with the 76 non-survivors showed that lower concentrations of DUPAN-2 (79.5 vs 312.5 U/mL, P = 0.032), tumor size ≤ 20 mm (35% vs 8%, P = 0.008), R0 resection (95% vs 61%, P = 0.004), and absence of lymph node metastases (60% vs 18%, P = 0.036) were significantly associated with the 5-year survival.
Conclusion: Negative surgical margins and a tumor size ≤ 20 mm were independent favorable prognostic factors. Histologically curative resection and early tumor detection are important factors in achieving long-term survival.
Keywords: Long-term survival; Long-term survivor; Pancreatic cancer; Prognostic factor; R0 resection.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Reber HA, Gloor B. Radical pancreatectomy. Surg Oncol Clin N Am. 1998;7:157–163. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, Brennan MF. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, Sauter PK, Coleman J, Hruban RH, Lillemoe KD. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
