

A new rat model of auxiliary partial heterotopic liver transplantation with liver dual arterial blood supply
- PMID: 25574199
- PMCID: PMC4280989
- DOI: 10.3892/etm.2014.2110
A new rat model of auxiliary partial heterotopic liver transplantation with liver dual arterial blood supply
Abstract
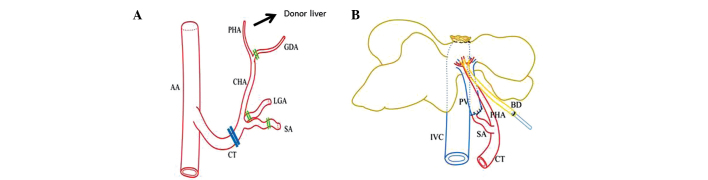
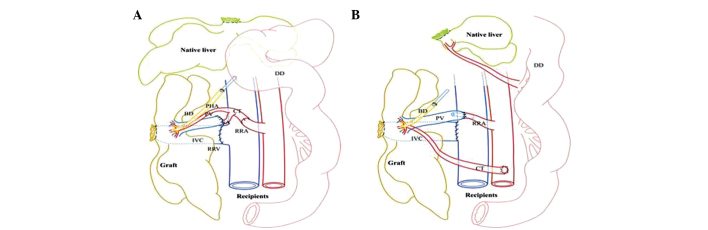
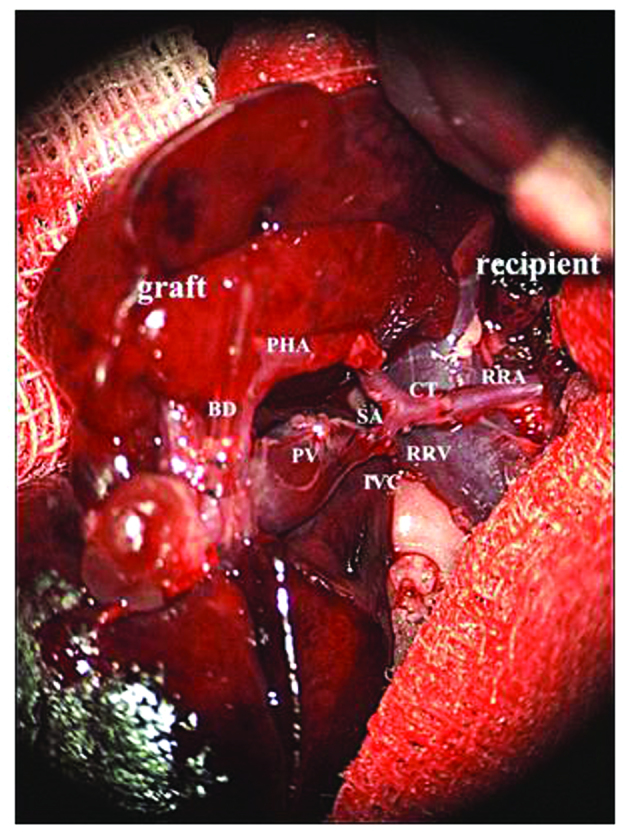
Auxiliary partial heterotopic liver transplantation (APHLT) with portal vein arterialization is a valuable procedure to be considered in the treatment of patients with acute liver failure and metabolic liver diseases. The aim of this study was to develop a new rat model of APHLT with liver dual arterial blood supply (LDABS). A total of 20 rats were used. The donor liver was resected, and the celiac trunk was reserved. Left and medial hepatic lobes accounting for 70% of the liver mass were removed en bloc and the suprahepatic caval vein was ligated simultaneously. Thus, 30% of the donor liver was obtained as the graft. Sleeve anastomosis of the graft portal vein and splenic artery were performed after narrowing the portal vein lumen through suturing. The right kidney of the recipient was removed, and sleeve anastomosis was performed between the celiac trunk of the graft and the right renal artery of the recipient. In addition, end-to-end anastomosis was performed between the infrahepatic caval vein of the graft and the right renal vein of the recipient. Following the reperfusion of the graft, the blood flow of the arterialized portal vein was controlled within the physiological range through suturing and narrowing under monitoring with an ultrasonic flowmeter. The bile duct of the graft was implanted into the duodenum of the recipient through an internal stent catheter. A 70% section of the native liver (left and medial hepatic lobes) was resected using bloodless hepatectomy. The mean operative duration was 154.5±16.4 min, and the warm and cold ischemia times of the graft were 8.1±1.1 min and 64.5±6.6 min, respectively. The blood flow of the arterialized portal vein to the graft was 1.8±0.3 ml/min/g liver weight. The success rate of model establishment (waking with post-surgical survival of >24 h) was 70% (7/10). Following successful model establishment, all rats survived 7 days post-surgery (100%; 7/7). The graft was found to be soft in texture and bright red in color following exploratory laparotomy. In conclusion, a new rat model of APHLT with LDABS without stent for vascular reconstruction was developed. This is a feasible and reliable rat model for liver transplantation study.
Keywords: auxiliary partial heterotopic liver transplantation; liver dual arterial blood supply; portal vein arterialization; rat.
Figures
References
-
- Jaeck D, Pessaux P, Wolf P. Which types of graft to use in patients with acute liver failure? (A) Auxiliary liver transplant (B) Living donor liver transplantation (C) The whole liver (A) I prefer auxiliary liver transplant. J Hepatol. 2007;46:570–573. doi: 10.1016/j.jhep.2007.01.012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials