

Mechanisms of Myofascial Pain
- PMID: 25574501
- PMCID: PMC4285362
- DOI: 10.1155/2014/523924
Mechanisms of Myofascial Pain
Abstract
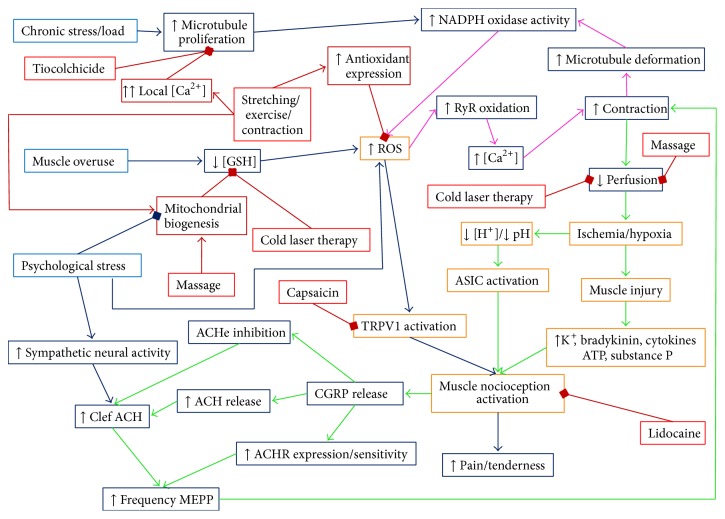
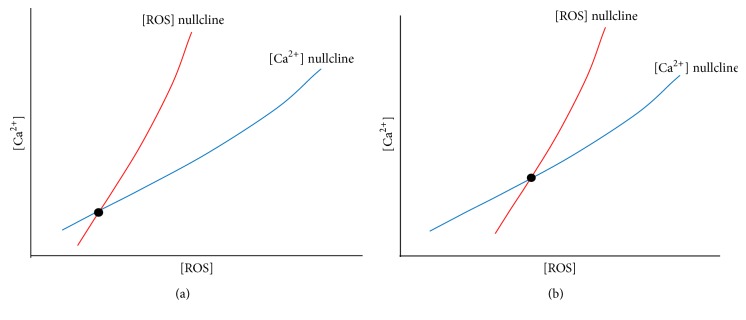
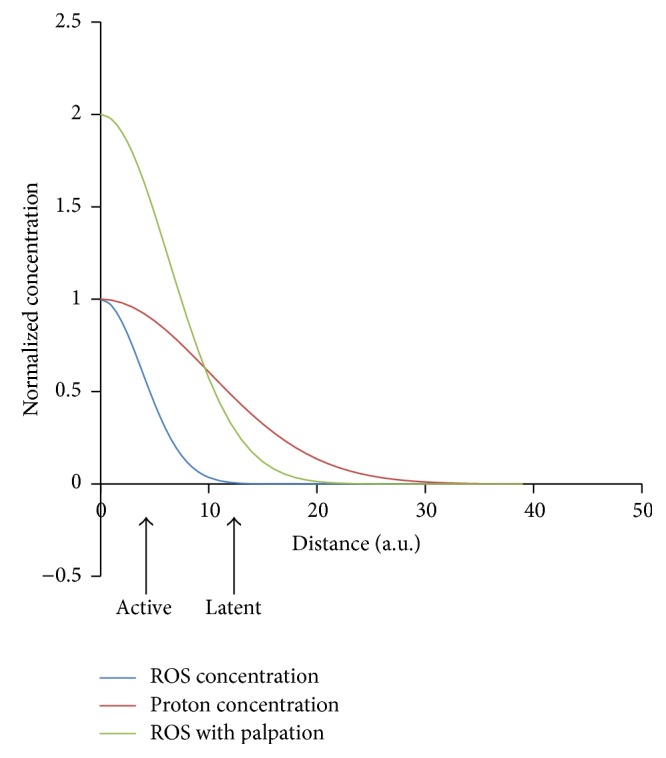
Myofascial pain syndrome is an important health problem. It affects a majority of the general population, impairs mobility, causes pain, and reduces the overall sense of well-being. Underlying this syndrome is the existence of painful taut bands of muscle that contain discrete, hypersensitive foci called myofascial trigger points. In spite of the significant impact on public health, a clear mechanistic understanding of the disorder does not exist. This is likely due to the complex nature of the disorder which involves the integration of cellular signaling, excitation-contraction coupling, neuromuscular inputs, local circulation, and energy metabolism. The difficulties are further exacerbated by the lack of an animal model for myofascial pain to test mechanistic hypothesis. In this review, current theories for myofascial pain are presented and their relative strengths and weaknesses are discussed. Based on new findings linking mechanoactivation of reactive oxygen species signaling to destabilized calcium signaling, we put forth a novel mechanistic hypothesis for the initiation and maintenance of myofascial trigger points. It is hoped that this lays a new foundation for understanding myofascial pain syndrome and how current therapies work, and gives key insights that will lead to the improvement of therapies for its treatment.
Figures
References
-
- Simons D. G. Clinical and etiological update of myofascial pain from trigger points. Journal of Musculoskeletal Pain. 1996;4(1-2):93–121. doi: 10.1300/J094v04n01_07. - DOI
-
- Fleckenstein J., Zaps D., Rüger L. J., et al. Discrepancy between prevalence and perceived effectiveness of treatment methods in myofascial pain syndrome: results of a cross-sectional, nationwide survey. BMC Musculoskeletal Disorders. 2010;11, article 32 doi: 10.1186/1471-2474-11-32. - DOI - PMC - PubMed
-
- Simons D. G ., Travell J. G., Simons L. S., Cummings B. D. Travell & Simons' Myofascial Pain and Dysfunction: The Trigger Point Manual. Lippincott Williams & Wilkins; 1998.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
