

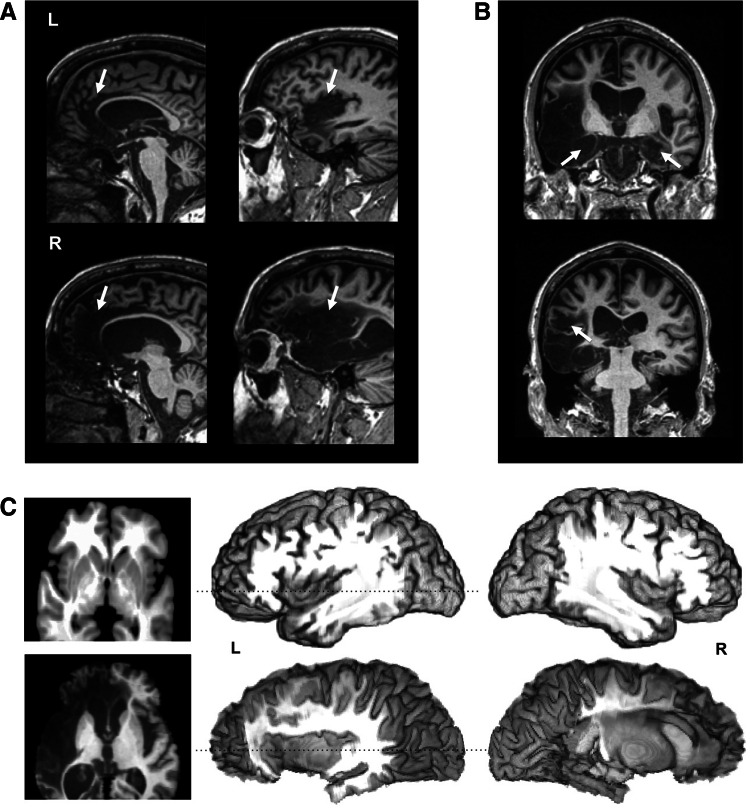
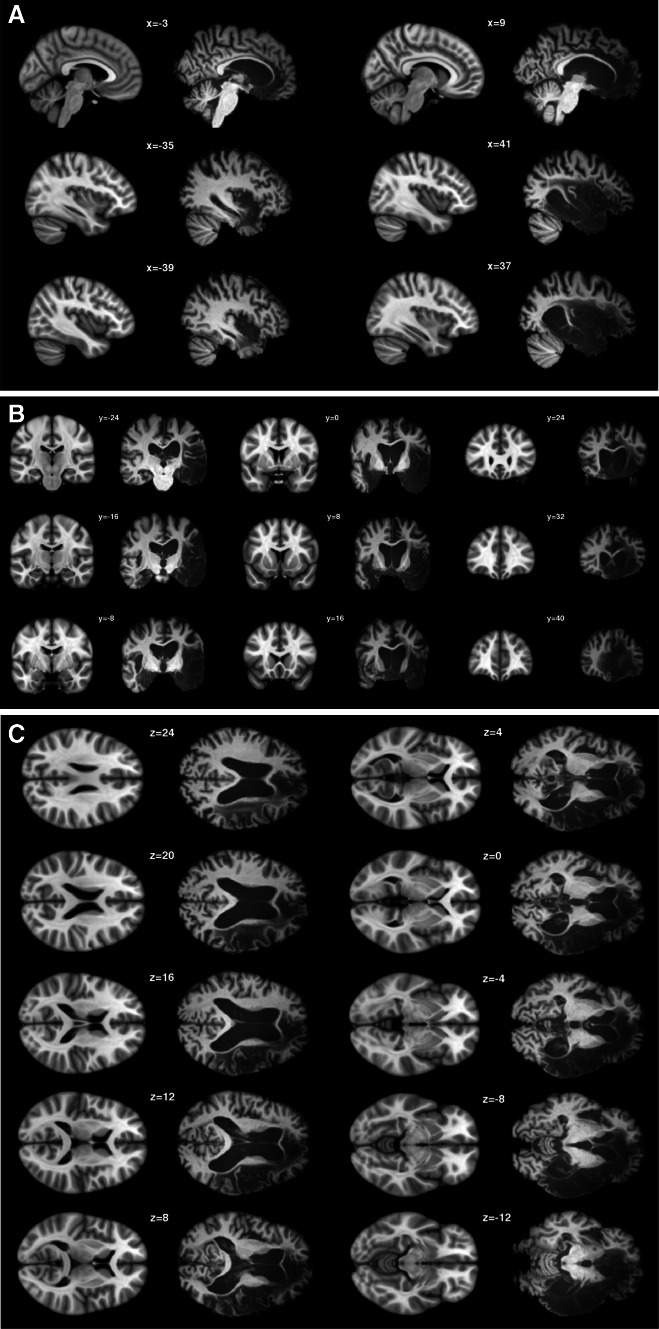
Preserved emotional awareness of pain in a patient with extensive bilateral damage to the insula, anterior cingulate, and amygdala
- PMID: 25577137
- PMCID: PMC4734900
- DOI: 10.1007/s00429-014-0986-3
Preserved emotional awareness of pain in a patient with extensive bilateral damage to the insula, anterior cingulate, and amygdala
Abstract
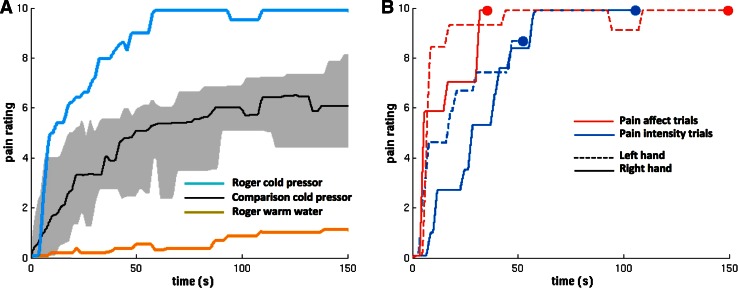
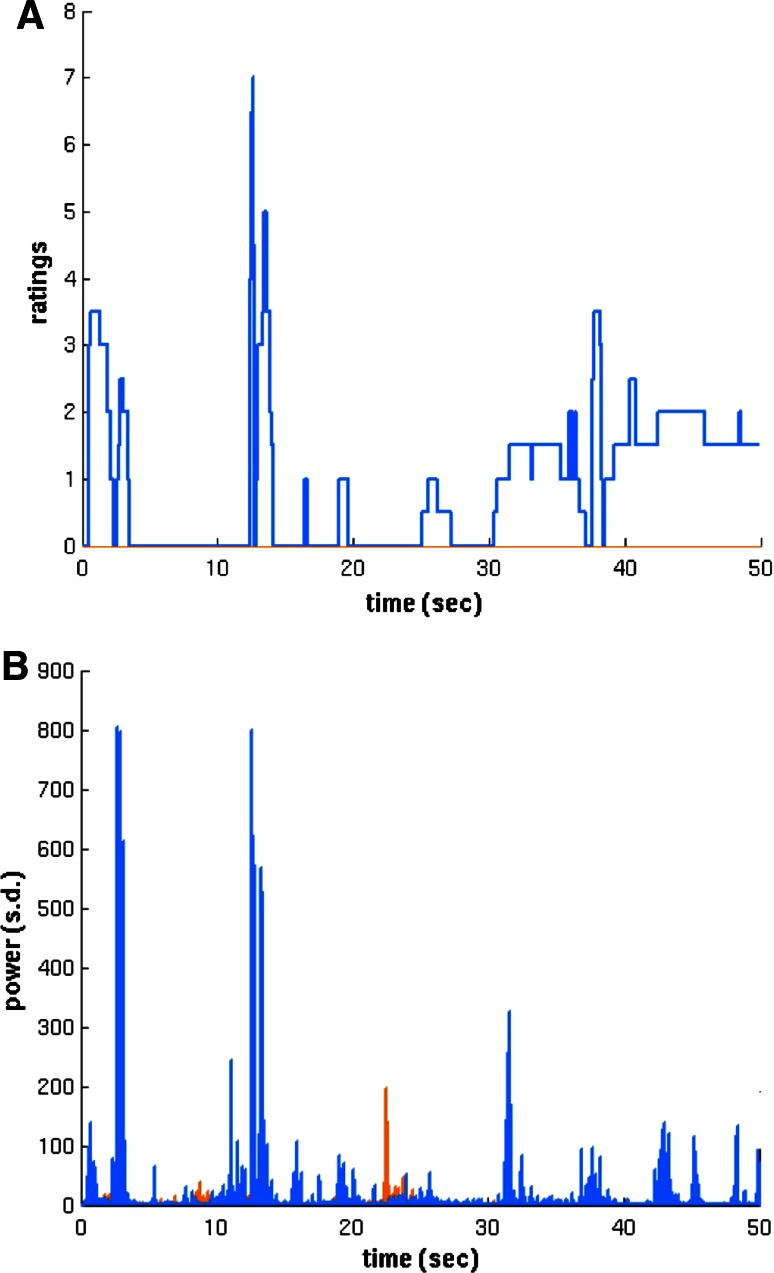
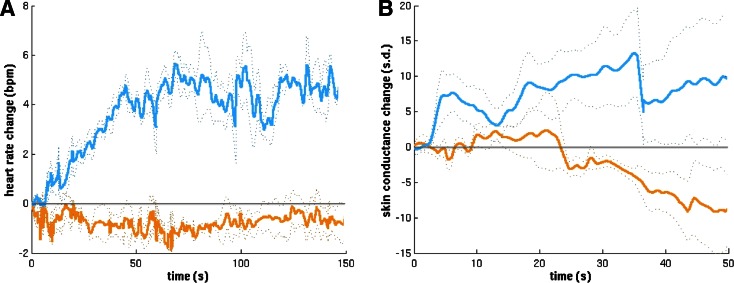
Functional neuroimaging investigations of pain have discovered a reliable pattern of activation within limbic regions of a putative "pain matrix" that has been theorized to reflect the affective dimension of pain. To test this theory, we evaluated the experience of pain in a rare neurological patient with extensive bilateral lesions encompassing core limbic structures of the pain matrix, including the insula, anterior cingulate, and amygdala. Despite widespread damage to these regions, the patient's expression and experience of pain was intact, and at times excessive in nature. This finding was consistent across multiple pain measures including self-report, facial expression, vocalization, withdrawal reaction, and autonomic response. These results challenge the notion of a "pain matrix" and provide direct evidence that the insula, anterior cingulate, and amygdala are not necessary for feeling the suffering inherent to pain. The patient's heightened degree of pain affect further suggests that these regions may be more important for the regulation of pain rather than providing the decisive substrate for pain's conscious experience.
Keywords: Brain lesion; Consciousness; Emotion; Feeling; Limbic system.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
