

Influence of childhood growth on asthma and lung function in adolescence
- PMID: 25577593
- PMCID: PMC4452091
- DOI: 10.1016/j.jaci.2014.10.046
Influence of childhood growth on asthma and lung function in adolescence
Abstract
Background: Low birth weight and rapid infant growth in early infancy are associated with increased risk of childhood asthma, but little is known about the role of postinfancy growth in asthmatic children.
Objectives: We sought to examine the associations of children's growth patterns with asthma, bronchial responsiveness, and lung function until adolescence.
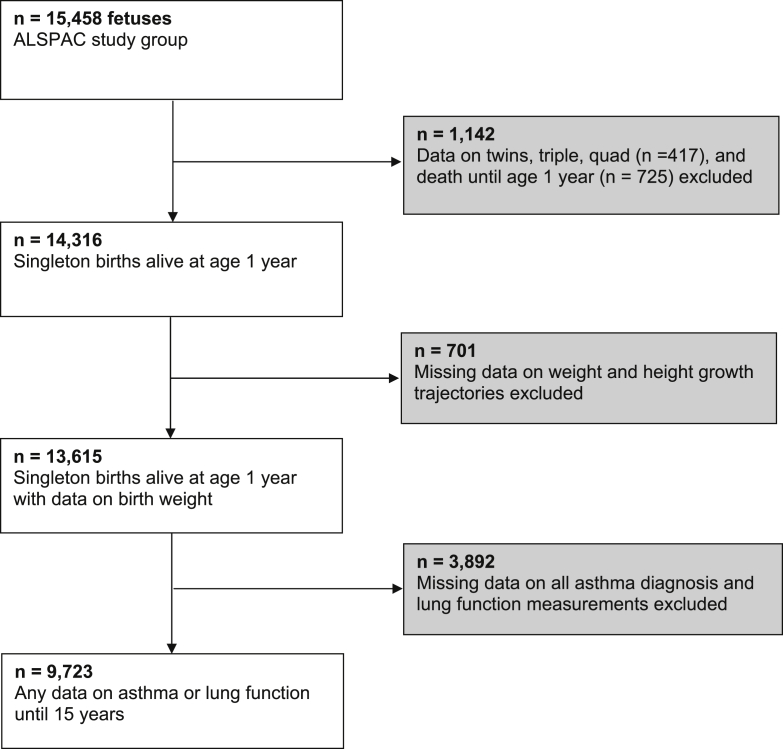
Methods: Individual growth trajectories from birth until 10 years of age were estimated by using linear spline multilevel models for 9723 children participating in a population-based prospective cohort study. Current asthma at 8, 14, and 17 years of age was based on questionnaires. Lung function and bronchial responsiveness or reversibility were measured during clinic visits at 8 and 15 years of age.
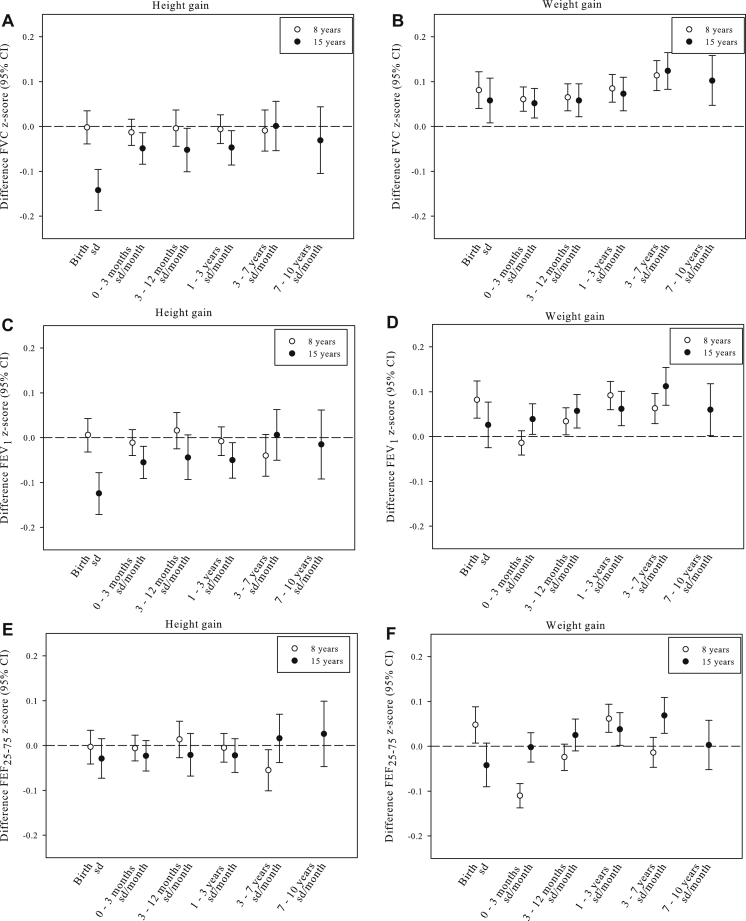
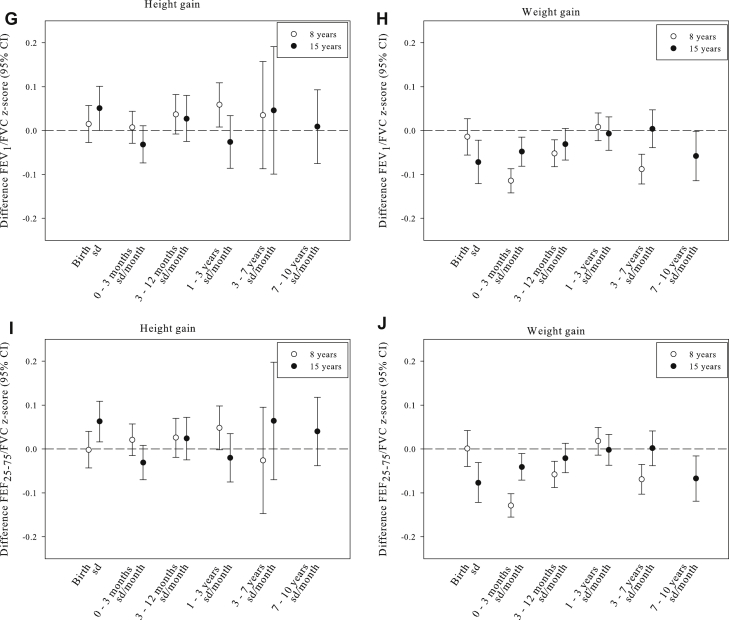
Results: Rapid weight growth between 0 and 3 months of age was most consistently associated with increased risks of current asthma at the ages of 8 and 17 years, bronchial responsiveness at age 8 years, and bronchial reversibility at age 15 years. Rapid weight growth was associated with lung function values, with the strongest associations for weight gain between 3 and 7 years of age and higher forced vital capacity (FVC) and FEV1 values at age 15 years (0.12 [95% CI, 0.08 to 0.17] and 0.11 [95% CI, 0.07 to 0.15], z score per SD, respectively) and weight growth between 0 and 3 months of age and lower FEV1/FVC ratios at age 8 and 15 years (-0.13 [95% CI, -0.16 to -0.10] and -0.04 [95% CI, -0.07 to -0.01], z score per SD, respectively). Rapid length growth was associated with lower FVC and FVC1 values at age 15 years.
Conclusion: Faster weight growth in early childhood is associated with asthma and bronchial hyperresponsiveness, and faster weight growth across childhood is associated with higher FVC and FEV1 values.
Keywords: ALSPAC; asthma; cohort study; growth; lung function.
Copyright © 2014 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The effect of early growth patterns and lung function on the development of childhood asthma: a population based study.Thorax. 2018 Dec;73(12):1137-1145. doi: 10.1136/thoraxjnl-2017-211216. Epub 2018 Jul 31. Thorax. 2018. PMID: 30064992
-
Early growth characteristics and the risk of reduced lung function and asthma: A meta-analysis of 25,000 children.J Allergy Clin Immunol. 2016 Apr;137(4):1026-1035. doi: 10.1016/j.jaci.2015.08.050. Epub 2015 Nov 11. J Allergy Clin Immunol. 2016. PMID: 26548843
-
Fetal and Infant Growth Patterns and Risk of Lower Lung Function and Asthma. The Generation R Study.Am J Respir Crit Care Med. 2018 Jan 15;197(2):183-192. doi: 10.1164/rccm.201703-0631OC. Am J Respir Crit Care Med. 2018. PMID: 28930491
-
Trajectories of airflow limitation from childhood to early adulthood: an analysis of six population-based birth cohorts.Lancet Child Adolesc Health. 2025 Mar;9(3):172-183. doi: 10.1016/S2352-4642(25)00001-X. Lancet Child Adolesc Health. 2025. PMID: 39978992
-
Monitoring asthma in childhood: lung function, bronchial responsiveness and inflammation.Eur Respir Rev. 2015 Jun;24(136):204-15. doi: 10.1183/16000617.00003914. Eur Respir Rev. 2015. PMID: 26028633 Free PMC article. Review.
Cited by
-
Bottle Size and Weight Gain in Formula-Fed Infants.Pediatrics. 2016 Jul;138(1):e20154538. doi: 10.1542/peds.2015-4538. Epub 2016 Jun 7. Pediatrics. 2016. PMID: 27273748 Free PMC article. Clinical Trial.
-
How Is Adolescent Bone Mass and Density Influenced by Early Life Body Size and Growth? The Tromsø Study: Fit Futures-A Longitudinal Cohort Study From Norway.JBMR Plus. 2018 Jun 7;2(5):268-280. doi: 10.1002/jbm4.10049. eCollection 2018 Sep. JBMR Plus. 2018. PMID: 30283908 Free PMC article.
-
Pre-adolescence DNA methylation is associated with lung function trajectories from pre-adolescence to adulthood.Clin Epigenetics. 2021 Jan 6;13(1):5. doi: 10.1186/s13148-020-00992-5. Clin Epigenetics. 2021. PMID: 33407823 Free PMC article.
-
A clinician's guide to effects of obesity on childhood asthma and into adulthood.Expert Rev Respir Med. 2024 Oct;18(10):759-775. doi: 10.1080/17476348.2024.2403500. Epub 2024 Sep 16. Expert Rev Respir Med. 2024. PMID: 39257361 Review.
-
Key paediatric messages from the 2018 European Respiratory Society International Congress.ERJ Open Res. 2019 Apr 29;5(2):00241-2018. doi: 10.1183/23120541.00241-2018. eCollection 2019 Apr. ERJ Open Res. 2019. PMID: 31044141 Free PMC article.
References
-
- Asher M.I., Montefort S., Bjorksten B., Lai C.K., Strachan D.P., Weiland S.K. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368:733–743. - PubMed
-
- Masoli M., Fabian D., Holt S., Beasley R. Global Initiative for Asthma Program. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy. 2004;59:469–478. - PubMed
-
- Duijts L., Jaddoe V.W., van der Valk R.J., Henderson J.A., Hofman A., Raat H. Fetal exposure to maternal and paternal smoking and the risks of wheezing in preschool children: the Generation R Study. Chest. 2012;141:876–885. - PubMed
-
- Sonnenschein-van der Voort A.M., Jaddoe V.W., van der Valk R.J., Willemsen S.P., Hofman A., Moll H.A. Duration and exclusiveness of breastfeeding and childhood asthma-related symptoms. Eur Respir J. 2012;39:81–89. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
