

Systematic review and meta-analysis of the survival outcomes of first-line treatment options in high-risk prostate cancer
- PMID: 25578739
- PMCID: PMC5378991
- DOI: 10.1038/srep07713
Systematic review and meta-analysis of the survival outcomes of first-line treatment options in high-risk prostate cancer
Abstract
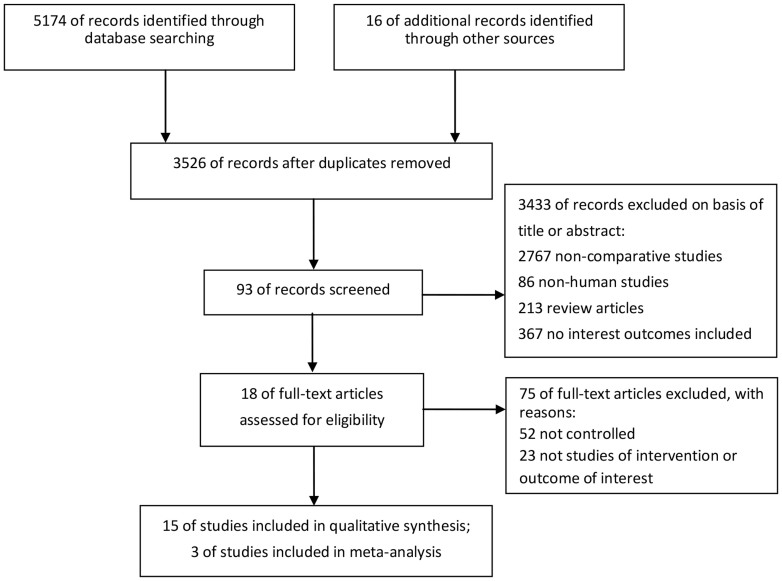
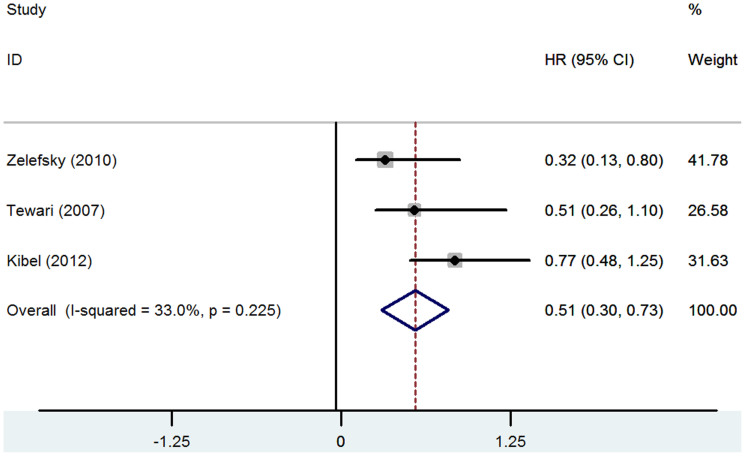
Prostate cancer (PCa) is the most common non-dermatologic cancer in the western countries in western countries. High-risk PCa accounts for 15% of the diagnosed cases. In this study, we compare the long-term survival outcomes of radical prostatectomy (RP), radiation therapy (RT), brachytherapy (BT), androgen- deprivation therapy (ADT), and watchful waiting (WW) in high-risk prostate cancer (PCa). Overall, RP/(RT plus ADT) gave the best survival outcome in patients with high-risk PCa, whereas ADT/WW had the worst outcome. The overall priority for treatment strategy could be ranked as follows: RP/(RT plus ADT), RT, and ADT/WW. RP had significant better overall survival (OS) than RT or BT, and RP had significant lower cancer-specific mortality (CSM) than RT (0.51 [95% CI 0.30-0.73], P<0.001). ADT improved the cancer-specific survival (CSS) of RP based on a case-controlled study; added ADT to RT failed to challenge the position of RP but could improve the outcome of RT. In conclusions,RP/(RT plus adjuvant ADT) could both be used for the first-line therapy of high-risk PCa. When encountering an individual patient, urologists should consider various factors like tumors themselves, preferences of individuals, and so on.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Bosetti C. et al. Trends in mortality from urologic cancers in Europe, 1970–2008. Eur Urol 60, 1–15 (2011). - PubMed
-
- Bastian P. J. et al. High-risk prostate cancer: from definition to contemporary management. Eur Urol 61, 1096–106 (2012). - PubMed
-
- D'Amico A. V. et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 280, 969–74 (1998). - PubMed
-
- Thompson I. et al. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol 177, 2106–31 (2007). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
