

Characteristics, management and outcomes of critically ill patients who are 80 years and older: a retrospective comparative cohort study
- PMID: 25580090
- PMCID: PMC4289550
- DOI: 10.1186/1471-2253-14-126
Characteristics, management and outcomes of critically ill patients who are 80 years and older: a retrospective comparative cohort study
Abstract
Background: Older age is associated with chronic illnesses and disability, which contribute to increased admission to the intensive care unit (ICU). Our primary objective was to compare the characteristics, ICU management and outcomes of critically ill patients ≥ 80 year-old with those of younger patients.
Methods: This was a retrospective cohort study of patients admitted to a tertiary-care ICU from 1999 to 2011. The characteristics, ICU management and outcomes of patients ≥ 80 year-old were compared with those 50-64.9 and 65-79.9 year-old. Multivariate analysis was performed to determine the adjusted risk of Do-Not-Resuscitate orders and hospital mortality in patients ≥ 80 year-old compared with the younger groups.
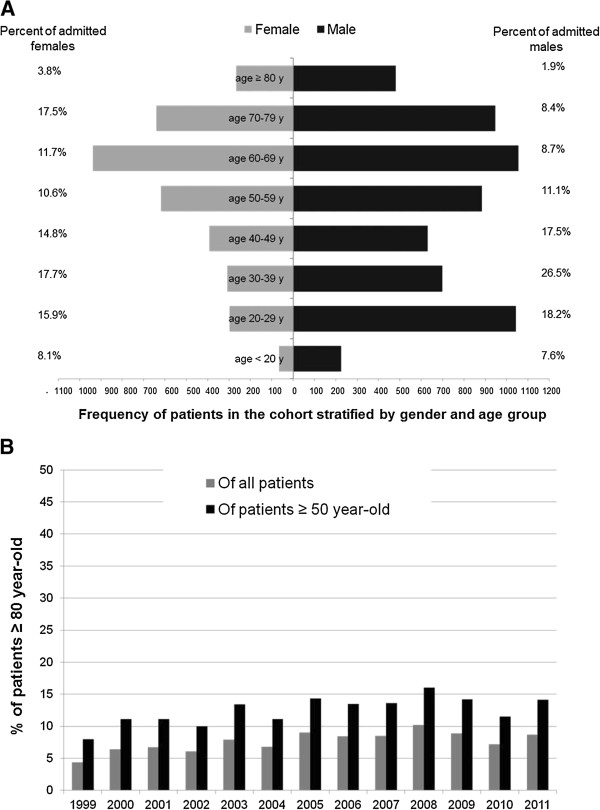
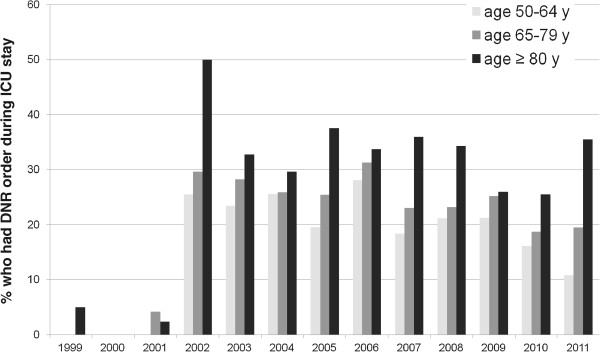
Results: During the study period, patients aged ≥ 80 years (N = 748) represented 7.9% of all ICU admissions and 12.8% of patients aged ≥ 50 years. Chronic cardiac (32.2%) and respiratory (21.8%) diseases were more prevalent in them than the younger groups (p < 0.0001). The most common reasons for their ICU admission were cardiovascular (30.9%) and respiratory (40.4%) conditions. Sepsis was commonly present in them on admission (32.9%). Mechanical ventilation and renal replacement therapy were commonly provided (76.9% and 16.0%, respectively). During ICU stay, Do-Not-Resuscitate orders were more frequently written for patients aged ≥ 80 years (35.0%) compared with 21.9% for 50-64.9 year-old group, p < 0.0001, and 25.4% for the 60-79.9 year-old group, p < 0.0001. On multivariate analysis, patients aged ≥ 80 years were more likely to receive these order compared with the 50-64.9 year-old patients (adjusted OR, 1.83; 95% CI, 1.45-2.31) and the 65-80 year-old patients (adjusted OR, 1.64; 95% CI, 1.32-2.04). The hospital mortality increased gradually with age and was highest (54.6%) in patients ≥ 80 year-old (p < 0.0001). Patients ≥ 80 year-old had higher risk of hospital mortality compared with patients aged 50-64.9 years (adjusted OR, 2.16; 95% CI, 1.73-2.69) and with those aged 65-79.9 years (adjusted OR, 1.51; 95% CI, 1.23-1.86).
Conclusions: Patients ≥ 80 year-old represented a significant proportion of ICU admissions. Although they received life sustaining measures similar to younger groups, they had higher adjusted mortality risk compared with the younger groups.
Keywords: Aged 80 and over; Critical illness; Health outcome; Mortality.
Figures

References
-
- Ewig S, Birkner N, Strauss R, Schaefer E, Pauletzki J, Bischoff H, Schraeder P, Welte T, Hoeffken G. New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality. Thorax. 2009;64(12):1062–1069. doi: 10.1136/thx.2008.109785. - DOI - PMC - PubMed
-
- Boumendil A, Angus DC, Guitonneau AL, Menn AM, Ginsburg C, Takun K, Davido A, Masmoudi R, Doumenc B, Pateron D, Garrouste-Orgeas M, Somme D, Simon T, Aegerter P, Guidet B, ICE-CUB study group Variability of intensive care admission decisions for the very elderly. PLoS One. 2012;7(4):e34387. doi: 10.1371/journal.pone.0034387. - DOI - PMC - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2253/14/126/prepub
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
