

Not always asthma: clinical and legal consequences of delayed diagnosis of laryngotracheal stenosis
- PMID: 25580336
- PMCID: PMC4281394
- DOI: 10.1155/2014/325048
Not always asthma: clinical and legal consequences of delayed diagnosis of laryngotracheal stenosis
Abstract
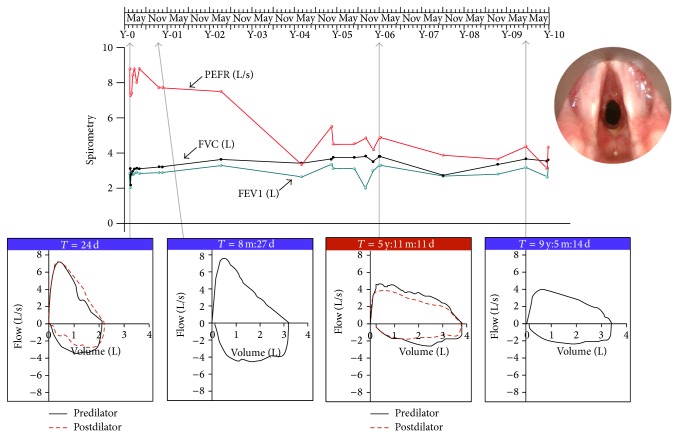
Laryngotracheal stenosis (LTS) is a rare condition that occurs most commonly as a result of instrumentation of the airway but may also occur as a result of inflammatory conditions or idiopathically. Here, we present the case of a patient who developed LTS as a complication of granulomatosis with polyangiitis (GPA), which was misdiagnosed as asthma for 6 years. After an admission with respiratory symptoms that worsened to the extent that she required intubation, a previously well 14-year-old girl was diagnosed with GPA. Following immunosuppressive therapy, she made a good recovery and was discharged after 22 days. Over subsequent years, she developed dyspnoea and "wheeze" and a diagnosis of asthma was made. When she became pregnant, she was admitted to hospital with worsening respiratory symptoms, whereupon her "wheeze" was correctly identified as "stridor," and subsequent investigations revealed a significant subglottic stenosis. The delay in diagnosis precluded the use of minimally invasive therapies, with the result that intermittent laser resection and open laryngotracheal reconstructive surgery were the only available treatment options. There were numerous points at which the correct diagnosis might have been made, either by proper interpretation of flow-volume loops or by calculation of the Empey or Expiratory Disproportion Indices from spirometry data.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
