

Risk factors for hospital and long-term mortality of critically ill elderly patients admitted to an intensive care unit
- PMID: 25580439
- PMCID: PMC4280808
- DOI: 10.1155/2014/960575
Risk factors for hospital and long-term mortality of critically ill elderly patients admitted to an intensive care unit
Abstract
Background: Data on long-term outcomes of elderly (≥65 years) patients in ICU are sparse.
Materials and methods: Adult patients (n = 1563, 45.4% elderly) admitted over 28 months were analyzed by competing risks regression model to determine independent factors related to in-hospital and long-term mortality.
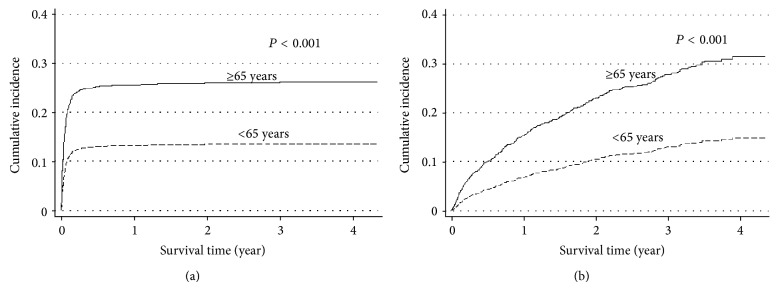
Results: 414 (26.5%) and 337 (21.6%) patients died in-hospital and during the 52 months following discharge, respectively; the elderly group had higher mortality during both periods. After discharge, elderly patients had 2.3 times higher mortality compared to the general population of the same age-group. In-hospital mortality was independently associated with mechanical ventilation (subdistribution hazard ratio (SHR) 2.74), vasopressors (SHR 2.56), neurological disease (SHR 1.77), and Mortality Prediction Model II score (SHR 1.01) regardless of age and with malignancy (SHR, hematological 3.65, nonhematological 3.4) and prior renal replacement therapy (RRT, SHR 2.21) only in the elderly. Long-term mortality was associated with low hemoglobin concentration (SHR 0.94), airway disease (SHR 2.23), and malignancy (SHR hematological 1.11, nonhematological 2.31) regardless of age and with comorbidities especially among the nonelderly.
Conclusions: Following discharge, elderly ICU patients have higher mortality compared to the nonelderly and general population. In the elderly group, prior RRT and malignancy contribute additionally to in-hospital mortality risk. In the long-term, comorbidities (age-related), anemia, airway disease, and malignancy were significantly associated with mortality.
Figures

References
-
- Department of Economic and Social Affairs, United Nations Population Division . World Population Ageing 1950–2050. New York, NY, USA: United Nations; 2012.
-
- Population trend 2012. Department of Statistics, Singapore, http://www.singstat.gov.sg/
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
