

Treatment for preventing tuberculosis in children and adolescents: a randomized clinical trial of a 3-month, 12-dose regimen of a combination of rifapentine and isoniazid
- PMID: 25580725
- PMCID: PMC6624831
- DOI: 10.1001/jamapediatrics.2014.3158
Treatment for preventing tuberculosis in children and adolescents: a randomized clinical trial of a 3-month, 12-dose regimen of a combination of rifapentine and isoniazid
Erratum in
-
Erratum in Table.JAMA Pediatr. 2015 Sep;169(9):878. doi: 10.1001/jamapediatrics.2015.2429. JAMA Pediatr. 2015. PMID: 26348861 No abstract available.
Abstract
Importance: Three months of a once-weekly combination of rifapentine and isoniazid for treatment of latent tuberculosis infection is safe and effective for persons 12 years or older. Published data for children are limited.
Objectives: To compare treatment safety and assess noninferiority treatment effectiveness of combination therapy with rifapentine and isoniazid vs 9 months of isoniazid treatment for latent tuberculosis infection in children.
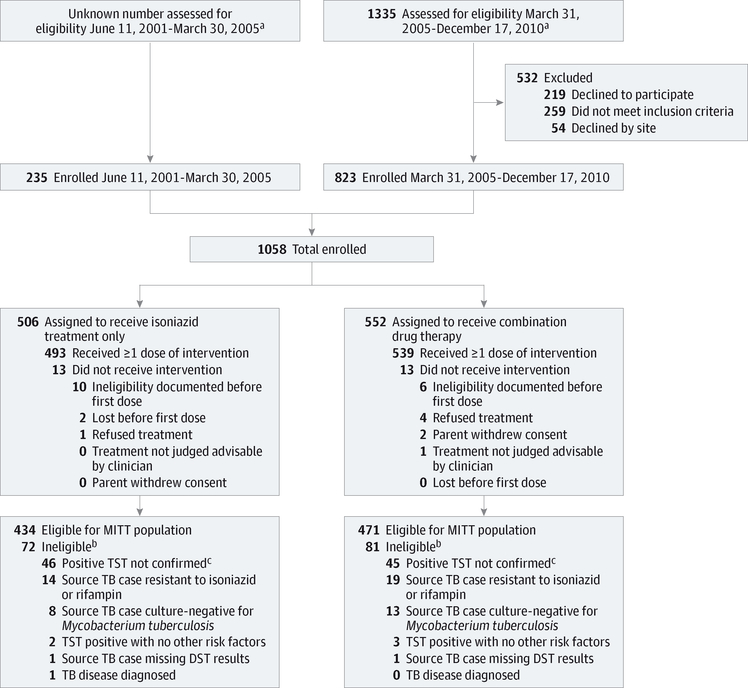
Design, setting, and participants: A pediatric cohort nested within a randomized, open-label clinical trial conducted from June 11, 2001, through December 17, 2010, with follow-up through September 5, 2013, in 29 study sites in the United States, Canada, Brazil, Hong Kong (China), and Spain. Participants were children (aged 2-17 years) who were eligible for treatment of latent tuberculosis infection.
Interventions: Twelve once-weekly doses of the combination drugs, given with supervision by a health care professional, for 3 months vs 270 daily doses of isoniazid, without supervision by a health care professional, for 9 months.
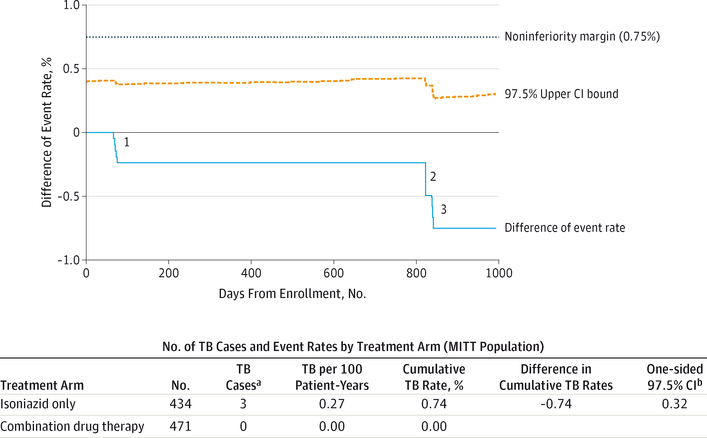
Main outcomes and measures: We compared rates of treatment discontinuation because of adverse events (AEs), toxicity grades 1 to 4, and deaths from any cause. The equivalence margin for the comparison of AE-related discontinuation rates was 5%. Tuberculosis disease diagnosed within 33 months of enrollment was the main end point for testing effectiveness. The noninferiority margin was 0.75%.
Results: Of 1058 children enrolled, 905 were eligible for evaluation of effectiveness. Of 471 in the combination-therapy group, 415 (88.1%) completed treatment vs 351 of 434 (80.9%) in the isoniazid-only group (P = .003). The 95% CI for the difference in rates of discontinuation attributed to an AE was -2.6 to 0.1, which was within the equivalence range. In the safety population, 3 of 539 participants (0.6%) who took the combination drugs had a grade 3 AE vs 1 of 493 (0.2%) who received isoniazid only. Neither arm had any hepatotoxicity, grade 4 AEs, or treatment-attributed death. None of the 471 in the combination-therapy group developed tuberculosis vs 3 of 434 (cumulative rate, 0.74%) in the isoniazid-only group, for a difference of -0.74% and an upper bound of the 95% CI of the difference of +0.32%, which met the noninferiority criterion.
Conclusions and relevance: Treatment with the combination of rifapentine and isoniazid was as effective as isoniazid-only treatment for the prevention of tuberculosis in children aged 2 to 17 years. The combination-therapy group had a higher treatment completion rate than did the isoniazid-only group and was safe.
Trial registration: clinicaltrials.gov Identifier: NCT00023452.
Conflict of interest statement
Figures
Comment in
-
Twelve-dose drug regimen now also an option for preventing tuberculosis in children and adolescents.JAMA Pediatr. 2015 Mar;169(3):208-10. doi: 10.1001/jamapediatrics.2014.3157. JAMA Pediatr. 2015. PMID: 25581905 No abstract available.
-
Intermittent Short Course Rifapentine-Isoniazid Combination for Preventing Tuberculosis in Children: Evidence based Medicine Viewpoint.Indian Pediatr. 2015 May;52(5):421-5. doi: 10.1007/s13312-015-0648-4. Indian Pediatr. 2015. PMID: 26061929 No abstract available.
References
-
- Swaminathan S, Rekha B. Pediatric tuberculosis: global overview and challenges. Clin Infect Dis. 2010;50(suppl 3):S184–S194. - PubMed
-
- World Health Organization. Global Tuberculosis Report 2012. Geneva, Switzerland: World Health Organization; 2012.
-
- Perez-Velez CM, Marais BJ. Tuberculosis in children. N Engl J Med. 2012;367(4):348–361. - PubMed
-
- Ferebee SH. An epidemiological model of tuberculosis in the United States. Bull Nat Tubercu Assoc. 1967;53:4–7.
-
- Heymann SJ, Brewer TF, Wilson ME, Colditz GA, Fineberg HV. Pediatric tuberculosis: what needs to be done to decrease morbidity and mortality. Pediatrics. 2000;106(1):1. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
