

Web-Based Access to Positive Airway Pressure Usage with or without an Initial Financial Incentive Improves Treatment Use in Patients with Obstructive Sleep Apnea
- PMID: 25581921
- PMCID: PMC4507728
- DOI: 10.5665/sleep.4898
Web-Based Access to Positive Airway Pressure Usage with or without an Initial Financial Incentive Improves Treatment Use in Patients with Obstructive Sleep Apnea
Abstract
Study objectives: We tested whether providing adults with obstructive sleep apnea (OSA) with daily Web-based access to their positive airway pressure (PAP) usage over 3 mo with or without a financial incentive in the first week improves adherence and functional outcomes.
Setting: Academic- and community-based sleep centers.
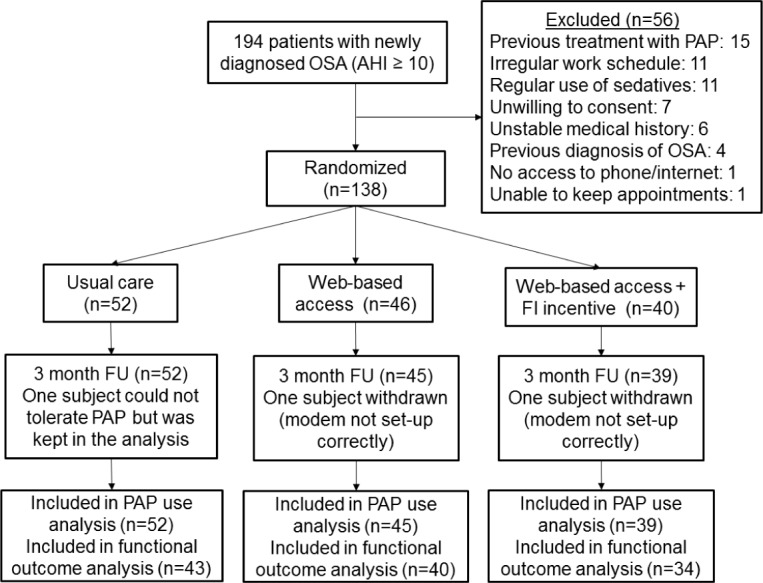
Participants: One hundred thirty-eight adults with newly diagnosed OSA starting PAP treatment.
Interventions: Participants were randomized to: usual care, usual care with access to PAP usage, or usual care with access to PAP usage and a financial incentive. PAP data were transmitted daily by wireless modem from the participants' PAP unit to a website where hours of usage were displayed. Participants in the financial incentive group could earn up to $30/day in the first week for objective PAP use ≥ 4 h/day.
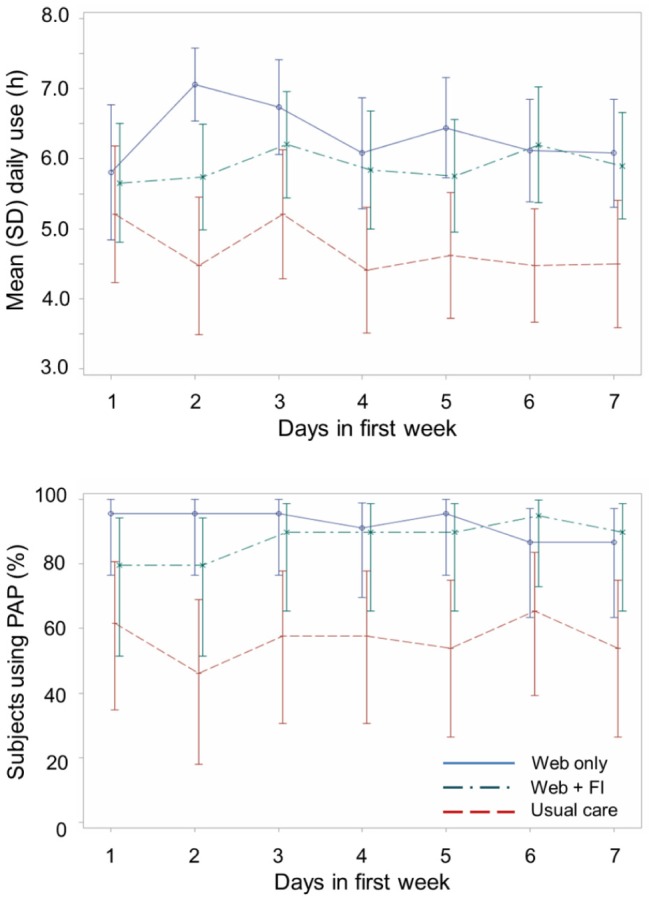
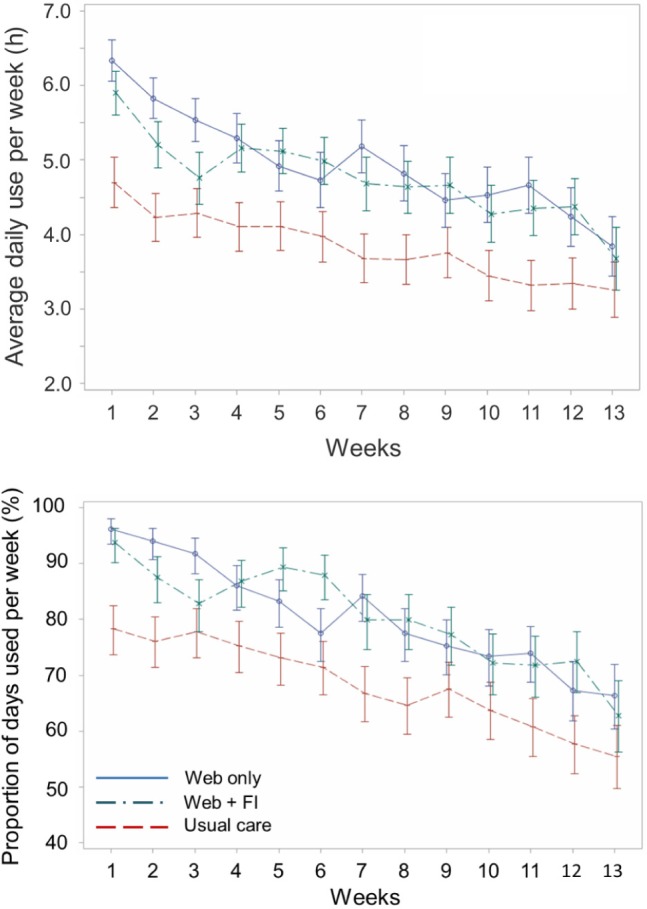
Measurements and results: Mean hours of daily PAP use in the two groups with access to PAP usage data did not differ from each other but was significantly greater than that in the usual care group in the first week and over 3 mo (P < 0.0001). Average daily use (mean ± standard deviation) during the first week of PAP intervention was 4.7 ± 3.3 h in the usual care group, and 5.9 ± 2.5 h and 6.3 ± 2.5 h in the Web access groups with and without financial incentive respectively. Adherence over the 3-mo intervention decreased at a relatively constant rate in all three groups. Functional Outcomes of Sleep Questionnaire change scores at 3 mo improved within each group (P < 0.0001) but change scores of the two groups with Web access to PAP data were not different than those in the control group (P > 0.124).
Conclusions: Positive airway pressure adherence is significantly improved by giving patients Web access to information about their use of the treatment. Inclusion of a financial incentive in the first week had no additive effect in improving adherence.
Keywords: adherence; internet; telehealth.
© 2015 Associated Professional Sleep Societies, LLC.
Figures
Comment in
-
Weaving the Internet of Sleep: The Future of Patient-Centric Collaborative Sleep Health Management Using Web-Based Platforms.Sleep. 2015 Aug 1;38(8):1157-8. doi: 10.5665/sleep.4882. Sleep. 2015. PMID: 26194574 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
