

What are incident reports telling us? A comparative study at two Australian hospitals of medication errors identified at audit, detected by staff and reported to an incident system
- PMID: 25583702
- PMCID: PMC4340271
- DOI: 10.1093/intqhc/mzu098
What are incident reports telling us? A comparative study at two Australian hospitals of medication errors identified at audit, detected by staff and reported to an incident system
Abstract
Objectives: To (i) compare medication errors identified at audit and observation with medication incident reports; (ii) identify differences between two hospitals in incident report frequency and medication error rates; (iii) identify prescribing error detection rates by staff.
Design: Audit of 3291 patient records at two hospitals to identify prescribing errors and evidence of their detection by staff. Medication administration errors were identified from a direct observational study of 180 nurses administering 7451 medications. Severity of errors was classified. Those likely to lead to patient harm were categorized as 'clinically important'.
Setting: Two major academic teaching hospitals in Sydney, Australia.
Main outcome measures: Rates of medication errors identified from audit and from direct observation were compared with reported medication incident reports.
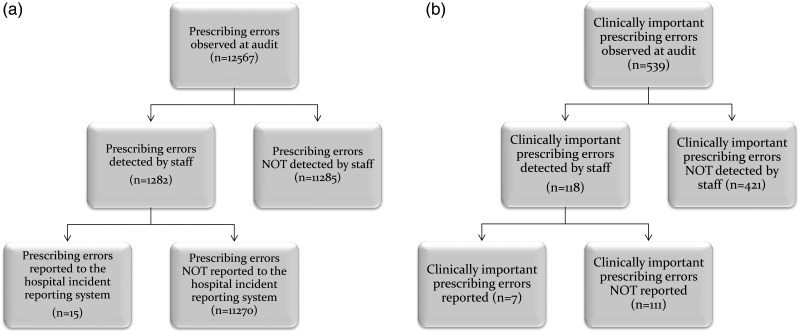
Results: A total of 12 567 prescribing errors were identified at audit. Of these 1.2/1000 errors (95% CI: 0.6-1.8) had incident reports. Clinically important prescribing errors (n = 539) were detected by staff at a rate of 218.9/1000 (95% CI: 184.0-253.8), but only 13.0/1000 (95% CI: 3.4-22.5) were reported. 78.1% (n = 421) of clinically important prescribing errors were not detected. A total of 2043 drug administrations (27.4%; 95% CI: 26.4-28.4%) contained ≥ 1 errors; none had an incident report. Hospital A had a higher frequency of incident reports than Hospital B, but a lower rate of errors at audit.
Conclusions: Prescribing errors with the potential to cause harm frequently go undetected. Reported incidents do not reflect the profile of medication errors which occur in hospitals or the underlying rates. This demonstrates the inaccuracy of using incident frequency to compare patient risk or quality performance within or across hospitals. New approaches including data mining of electronic clinical information systems are required to support more effective medication error detection and mitigation.
Keywords: electronic prescribing; incident reporting; medication administration errors; medication error; safety.
© The Author 2015. Published by Oxford University Press in association with the International Society for Quality in Health Care.
Figures
References
-
- Fitzgerald E, Cawley D, Rowan N. Irish staff nurses’ perceptions of clinical incident reporting. Int J Nurs Midwifery. 2011;3:14–21.
-
- Farley DO, Haviland A, Champagne S, et al. Adverse-event-reporting practices by US hospitals: results of a national survey. Qual Saf Health Care. 2008;17:416–23. - PubMed
-
- Farley DO, Haviland A, Haas A, et al. How event reporting by US hospitals has changed from 2005 to 2009. BMJ Qual Saf. 2012;21:70–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
