

The clinical role and cost-effectiveness of long-acting antiretroviral therapy
- PMID: 25583979
- PMCID: PMC4366583
- DOI: 10.1093/cid/ciu1159
The clinical role and cost-effectiveness of long-acting antiretroviral therapy
Abstract
Background: Long-acting antiretroviral therapy (LA-ART) is currently under development and could improve outcomes for human immunodeficiency virus (HIV)-infected individuals with poor daily ART adherence.
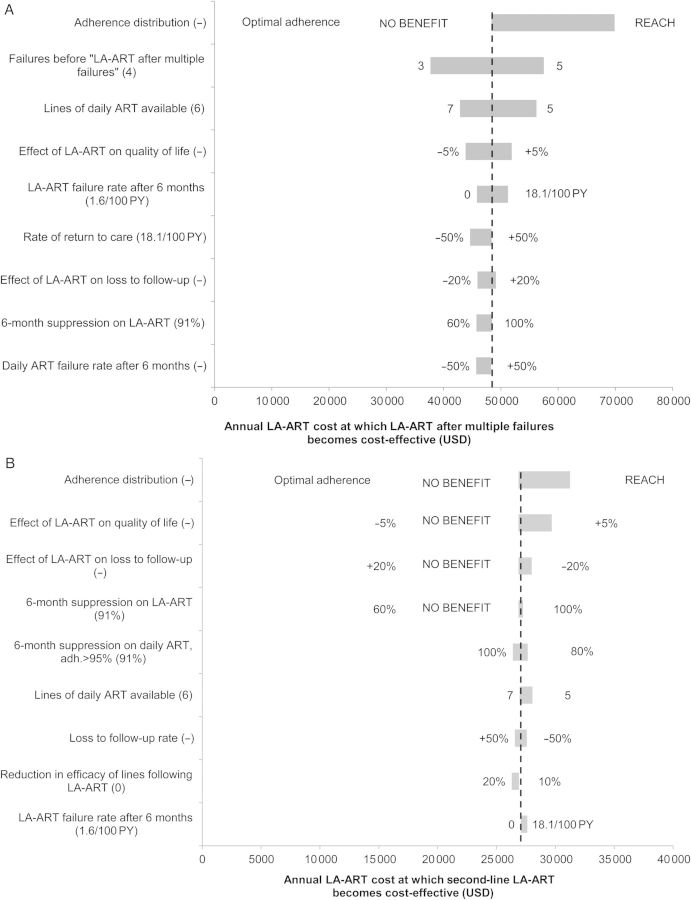
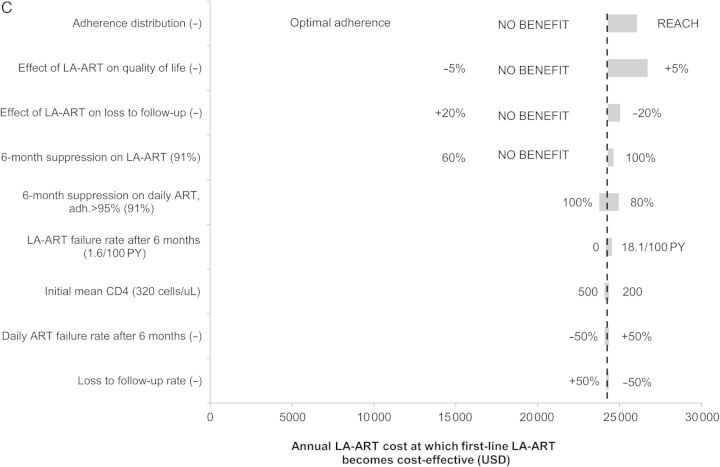
Methods: We used a computer simulation model to evaluate the cost-effectiveness of 3 LA-ART strategies vs daily oral ART for all: (1) LA-ART for patients with multiple ART failures; (2) second-line LA-ART for those failing first-line therapy; and (3) first-line LA-ART for ART-naive patients. We calculated the maximum annual cost of LA-ART at which each strategy would be cost-effective at a willingness to pay of $100 000 per quality-adjusted life-year. We assumed HIV RNA suppression on daily ART ranged from 0% to 91% depending on adherence, vs 91% suppression on LA-ART regardless of daily ART adherence. In sensitivity analyses, we varied adherence, efficacy of LA-ART and daily ART, and loss to follow-up.
Results: Relative to daily ART, LA-ART increased overall life expectancy by 0.15-0.24 years, and by 0.51-0.89 years among poorly adherent patients, depending on the LA-ART strategy. LA-ART after multiple failures became cost-effective at an annual drug cost of $48 000; in sensitivity analysis, this threshold varied from $40 000-$70 000. Second-line LA-ART and first-line LA-ART became cost-effective at an annual drug cost of $26 000-$31 000 and $24 000-$27 000, vs $28 000 and $25 000 for current second-line and first-line regimens.
Conclusions: LA-ART could improve survival of HIV patients, especially those with poor daily ART adherence. At an annual cost of $40 000-$70 000, LA-ART will offer good value for patients with multiple prior failures. To be a viable option for first- or second-line therapy, however, its cost must approach that of currently available regimens.
Keywords: HIV/AIDS; cost-effectiveness; long-acting antiretroviral therapy; modeling.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Cost-effectiveness of first-line antiretroviral therapy for HIV-infected African children less than 3 years of age.AIDS. 2015 Jun 19;29(10):1247-59. doi: 10.1097/QAD.0000000000000672. AIDS. 2015. PMID: 25870982 Free PMC article.
-
Does combining antiretroviral agents in a single dosage form enhance quality of life of HIV/AIDS patients? A cost-utility study.Res Social Adm Pharm. 2012 Mar-Apr;8(2):157-65. doi: 10.1016/j.sapharm.2010.12.004. Epub 2011 Jun 28. Res Social Adm Pharm. 2012. PMID: 21712147
-
Cost-effectiveness of HIV treatment in resource-poor settings--the case of Côte d'Ivoire.N Engl J Med. 2006 Sep 14;355(11):1141-53. doi: 10.1056/NEJMsa060247. N Engl J Med. 2006. PMID: 16971720
-
The lifetime cost of current human immunodeficiency virus care in the United States.Med Care. 2006 Nov;44(11):990-7. doi: 10.1097/01.mlr.0000228021.89490.2a. Med Care. 2006. PMID: 17063130 Review.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
Cited by
-
Modeling the health impact and cost threshold of long-acting ART for adolescents and young adults in Kenya.EClinicalMedicine. 2020 Jul 16;25:100453. doi: 10.1016/j.eclinm.2020.100453. eCollection 2020 Aug. EClinicalMedicine. 2020. PMID: 32954235 Free PMC article.
-
Cost-effectiveness of the long-acting regimen cabotegravir plus rilpivirine for the treatment of HIV-1 and its potential impact on adherence and viral transmission: A modelling study.PLoS One. 2021 Feb 2;16(2):e0245955. doi: 10.1371/journal.pone.0245955. eCollection 2021. PLoS One. 2021. PMID: 33529201 Free PMC article.
-
Projected Life Expectancy Gains From Improvements in HIV Care in Black and White Men Who Have Sex With Men.JAMA Netw Open. 2023 Nov 1;6(11):e2344385. doi: 10.1001/jamanetworkopen.2023.44385. JAMA Netw Open. 2023. PMID: 38015507 Free PMC article.
-
Access to a novel first-line single-tablet HIV antiretroviral regimen in Affordable Care Act Marketplace plans, 2018-2020.J Pharm Policy Pract. 2023 Apr 20;16(1):57. doi: 10.1186/s40545-023-00559-8. J Pharm Policy Pract. 2023. PMID: 37081570 Free PMC article.
-
Survival benefits of antiretroviral therapy in Brazil: a model-based analysis.J Int AIDS Soc. 2016 Mar 29;19(1):20623. doi: 10.7448/IAS.19.1.20623. eCollection 2016. J Int AIDS Soc. 2016. PMID: 27029828 Free PMC article.
References
-
- Walensky RP, Paltiel AD, Losina E, et al. The survival benefits of AIDS treatment in the United States. J Infect Dis. 2006;194:11–9. - PubMed
-
- Wood E, Hogg RS, Yip B, Harrigan PR, O'Shaughnessy MV, Montaner JSG. Effect of medication adherence on survival of HIV-infected adults who start highly active antiretroviral therapy when the CD4(+) cell count is 0.200 to 0.350 X 10(9) cells/L. Ann Intern Med. 2003;139:810–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
