

Geriatric trauma hip fractures: is there a difference in outcomes based on fracture patterns?
- PMID: 25584064
- PMCID: PMC4290806
- DOI: 10.1186/1749-7922-9-59
Geriatric trauma hip fractures: is there a difference in outcomes based on fracture patterns?
Abstract
Background: Annually in the US, there are over 300,000 hospital admissions due to hip fractures in geriatric patients. Consequently, there have been several large observational studies, which continue to provide new insights into differences in outcomes among hip fracture patients. However, few hip fracture studies have specifically examined the relationship between hip fracture patterns, sex, and short-term outcomes including hospital length of stay and discharge disposition in geriatric trauma patients.
Methods: We performed a retrospective study of hip fractures in geriatric trauma patients. Hip fracture patterns were based on ICD -9 CM diagnostic codes for hip fractures (820.00-820.9). Patient variables were patient demographics, mechanism of injury, injury severity score, hospital and ICU length of stay, co-morbidities, injury location, discharge disposition, and in-patient mortality.
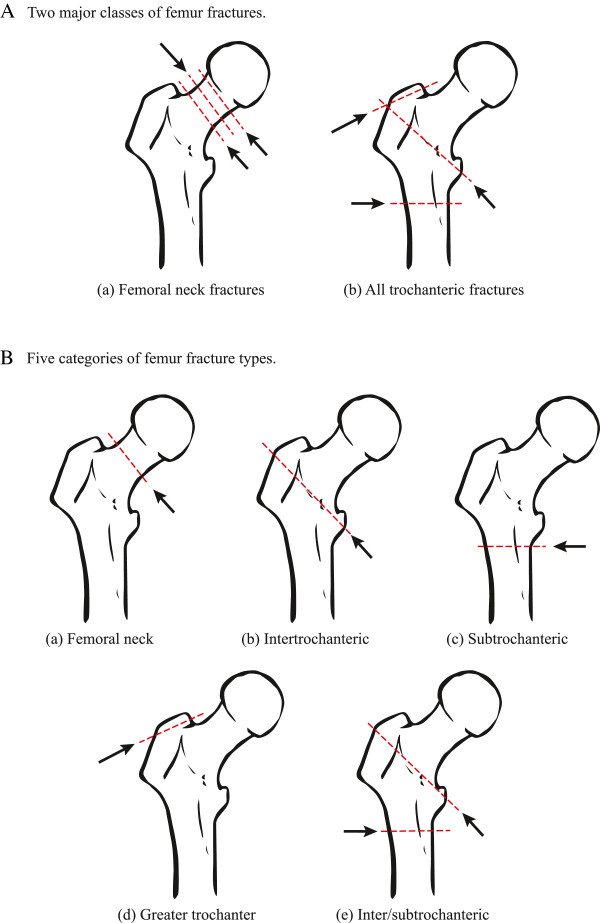
Results: A total of 325 patient records met the inclusion criteria. The mean age of the patients was 82.2 years, and the majority of the patients were white (94%) and female (70%). Hip fractures patterns were categorized as two fracture classes and three fracture types. We observed a difference in the proportion of males to females within each fracture class (Femoral neck fractures Z-score = -8.86, p < 0.001, trochanteric fractures Z-score = -5.63, p < 0.001). Hip fractures were fixed based on fracture pattern and patient characteristics. Hip fracture class or fracture type did not predict short-term outcomes such as in-hospital or ICU length of stay, death, or patient discharge disposition. The majority of patients (73%) were injured at home. However, 84% of the patients were discharged to skilled nursing facility, rehabilitation, or long-term care while only 16% were discharged home. There was no evidence of significant association between fracture pattern, injury severity score, diabetes mellitus, hypertension or dementia.
Conclusions: Hip fracture patterns differ between geriatric male and female trauma patients. However, there was no significant association between fracture patterns and short-term patient outcomes. Further studies are planned to investigate the effect of fracture pattern and long-term outcomes including 90-day mortality, return to previous levels of activity, and other quality of life measures.
Keywords: Femoral neck fractures; Geriatric G-60; Hip fracture patterns; Hip fractures; Length of stay.
Figures



References
-
- Bentler SE, Liu L, Obrizan M, Cook EA, Wright KB, Geweke JF, Chrischilles EA, Pavlik CE, Wallace RB, Ohsfeldt RL, Jones MP, Rosenthal GE, Wolinsky FD. The aftermath of hip fracture: discharge placement, functional status change, and mortality. Am J Epidemiol. 2009;170:1290–1299. doi: 10.1093/aje/kwp266. - DOI - PMC - PubMed
-
- Cummings SR, Rubin SM, Black D. The future of hip fractures in the United States. Numbers, costs, and potential effects of postmenopausal estrogen. Clin Orthop Relat Res. 1990;252:163–166. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
